Article Text

Statistics from Altmetric.com
According to cancer research UK, bladder cancer is the seventh most common cancer in the UK. Affecting more men than woman, with smoking being a major preventable risk factor. Urothelial tumours fall into three separate categories of tumour characteristics; non-invasive, muscle invasive, and metastatic disease. Vinflunine is only for the treatment of urothelial (transitional cell) bladder cancer; other medications are used in the treatment of non-urothelial bladder cancer or small cell carcinoma of the urethra.
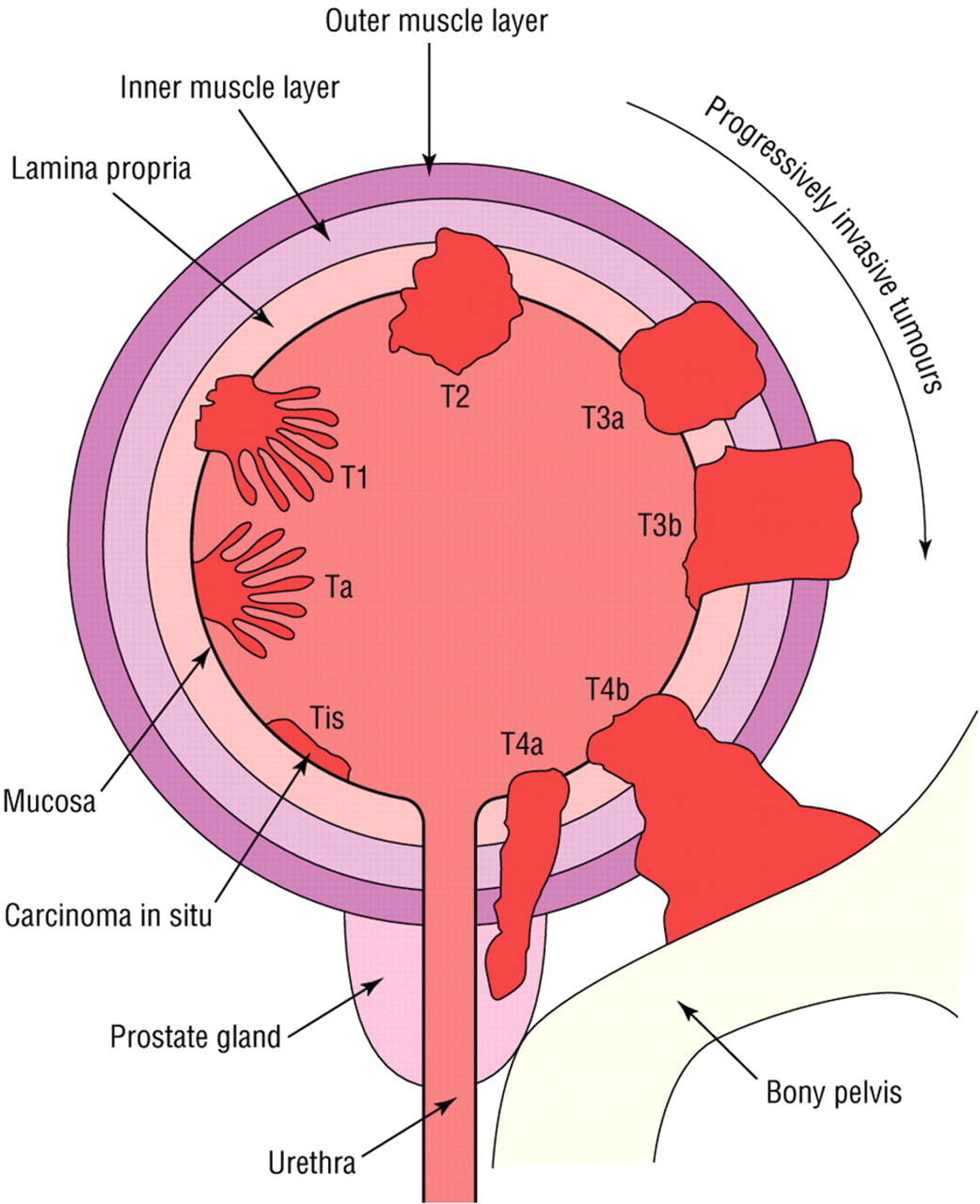
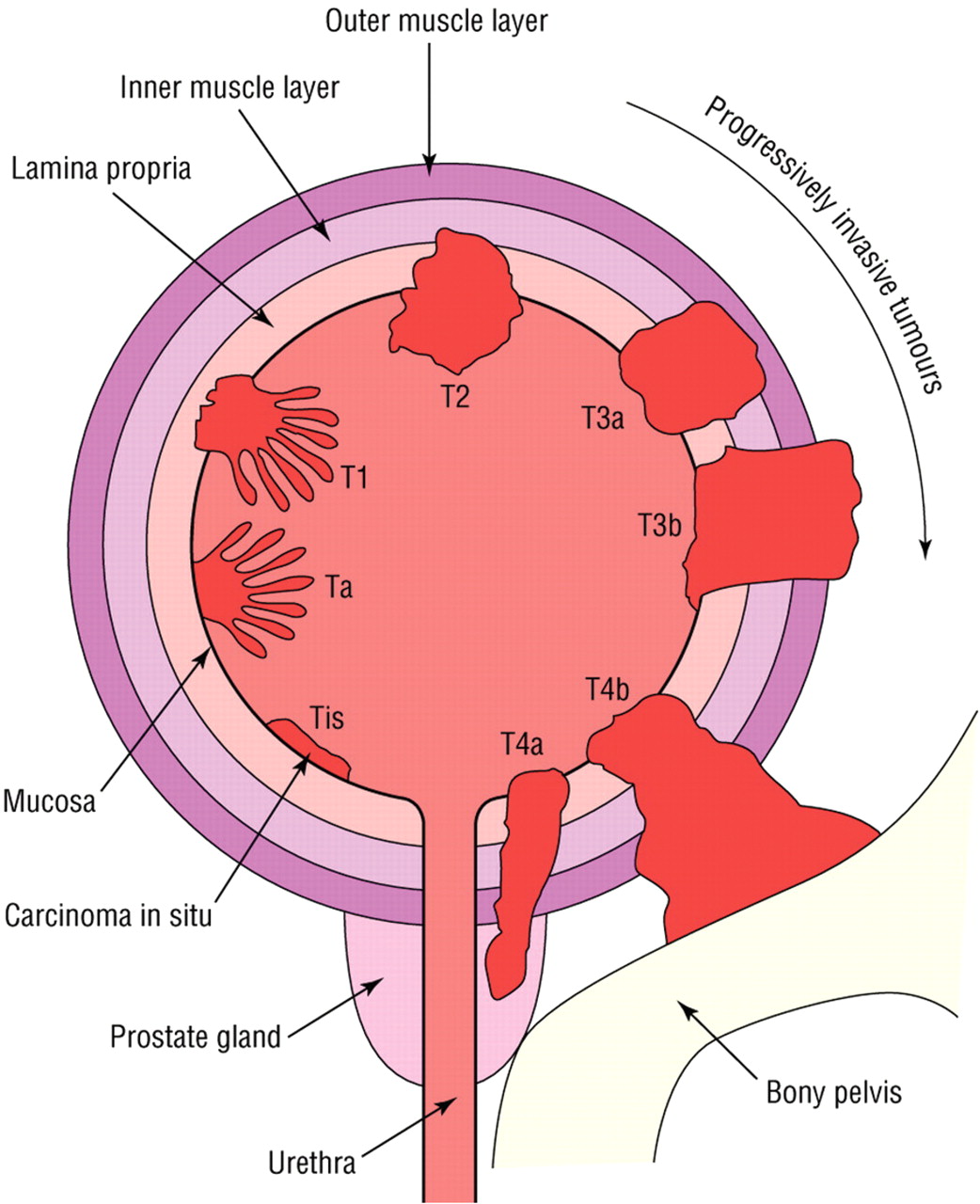
Patients often present with painless haematuria. They are typically over 65 years old. Prognosis of overall survival has a high correlation to the depth of invasion of the tumour into the outlying area. See figure 1 for classification of bladder cancer by the tumour, node, metastasis system.
{kind=link}
T-staging of bladder cancer.
Management depends on the severity of the diagnosis. For non-invasive disease.
Low risk disease will usually be treated by transurethral resection of bladder tumour, followed by a one time dose of chemotherapy. Some patients with more severe disease may qualify to have intravesical treatment with Bacillus Calmette Guerin or Mitomycin C in an attempt to kill any remaining tumour cells and tumour implantation. Patients with muscle invasive tumours or relapse will likely be candidates for cystectomy.
Chemotherapy is often used in those patients who have locally inoperable advanced or metastatic disease. In these patients, using a platinum based regime combining methotrexate, vinblastine, doxorubicine and cisplatin is first line therapy. Gemcitabine and paclitaxel are additional agents that may be combined with cisplatin in the treatment of bladder cancer. Unfortunately, even though these regimes are able to significantly reducing the tumour load, they have had only marginal benefit in long term survival. According to cancer research UK, the average life expectancy in metastatic bladder cancer is 18 months with aggressive treatment as compared to 6 months without treatment. Only 15% of patients with metastatic bladder cancer will survive more than 5 years.
The statistics for this scenario is pretty grim and recently the National Institute for Health and Clinical Excellence (NICE) rejected vinflunine as a formulary item due to cost and impact on market. It is estimated that the cost per quality adjusted life year gained with the use of Javlor is more than £120 000. Several comparative studies for treatment of bladder cancer have been terminated prematurely due to the inability of the studies to get adequate power in order to determine statistical significance. What is true is that vinflunine acts similar to other vinca alkaloids. It may cause less neurotoxicity than the others but NICE does not find this benefit being worth the cost.
Snap shot
Vinflunine (Javlor)
Manufacturer: Pierre Fabre Medicament
Drug Class:Vinca alkaloids and analogues, ATC code L01CA05
Indication:Monotherapy for the treatment of adult patients with advanced or metastatic transitional cell carcinoma of the urothelial tract after failure of a prior platinum-containing regimen.
Posology:320 mg/m2 vinflunine as a 20 min intravenous infusion every 3 weeks. Dose adjustments are necessary based on toxicity, renal and hepatic impairment.
Of special note:
*Vinflunine must only be administered intravenously. Intrathecal administration of
vinflunine may be fatal!
*Either peripheral lines or a central catheter can be used for vinflunine administration.
*Laxatives and dietary measures including oral hydration are recommended from day 1 to day 5 or 7 after each administration.
*Avoid concomitant use of opioids due to enhanced risk of constipation.
*Complete blood counts are needed to verify Absolute Neutrophil Count value before each vinflunine infusion due to the high incidence of neutropenia.
*Avoid co-administration of potent CYP3A4 inhibitors (ie, ketoconazole, ritonavir and grapefruit juice) or inducers (ie, rifampicine and St John's wort) which may result in an increase or decrease of vinflunine levels.
*Store in refrigerator (2–8°C)
*Store in the original package in order to protect from light.
*Diluted solution should be used immediately. Keep protected from light and the reconstituted product may be refrigerated (2–8°C) for 6 days and 24 h at 25°C. Unprotected from light for 1 h at 25°C.
Method of administering
▶ A venous access for a 500 ml bag of sodium chloride (NaCl) 0.9% solution for injection or glucose 5% solution for infusion
▶ Upper part of the forearm or central venous arm
▶ The veins of the hand dorsum and those close to joints should be avoided
▶ The IV should start with half of the 500 ml bag of NaCl 0.9% for infusion or of glucose 5% solution for infusion, that is, 250 ml, at a free flowing rate to flush the vein
▶ The vinflunine solution for infusion should be piggy-backed to the side injection port closest to the 500 ml bag to further dilute vinflunine.
▶ The patency should be assessed frequently and extravasation precautions should be maintained throughout the infusion
▶ After vinflunine infusion is completed, the remaining 250 ml from the NaCl 0.9% solution for infusion or of glucose 5% solution for infusion bag should be run at a flowing rate of 300 ml/h. In order to flush the vein, administration of vinflunine solution for infusion should always be followed by at least an equal volume of NaCl 0.9% solution for infusion or of glucose 5% solution for infusion.
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.