Article Text

Statistics from Altmetric.com
Background
As people get older, polypharmacy increases and there is an increased risk of adverse drug events, drug interactions, low medication adherence, increasing economic burden, hospital admissions and even drug-related deaths.1 It has also been stated that the problems of inappropriate pharmacotherapy are expected to grow in the future as new drugs are introduced, new uses for old drugs are found and as the population lives longer with an increased risk of chronic medical conditions. Poor communication of medical information suggests that 40 –85% of elderly patients have at least one error in their medications when they are transferred between primary and hospital care.2–6 In order to improve quality in the use of medications in society, and for individual patients, there is a need to identify problems and errors in structures and processes to improve the outcome of care and to reduce errors.7
A systematic analysis of potential problems and limitations during the standard patient medication care process was performed by the Drug and Therapeutics Committee at Lund University Hospital in 1999. This followed admission, hospital stay and post discharge. After confirmation of the problems, a project was initiated. The aim was to build a model based on systematic training, activities and responsibilities, to identify, solve and prevent drug related problems (DRPs) in the healthcare process, starting from when a patient is admitted to hospital. For patient based clinical pharmacy services, we identified no systematic research or models focusing on all of these aspects.
Herein is an overview of the results which have been published in 17 separate publications.2–6 8–19 Readers are encouraged to follow-up specific results by referring to tables 2 and 3 for the referenced summary.
Methods
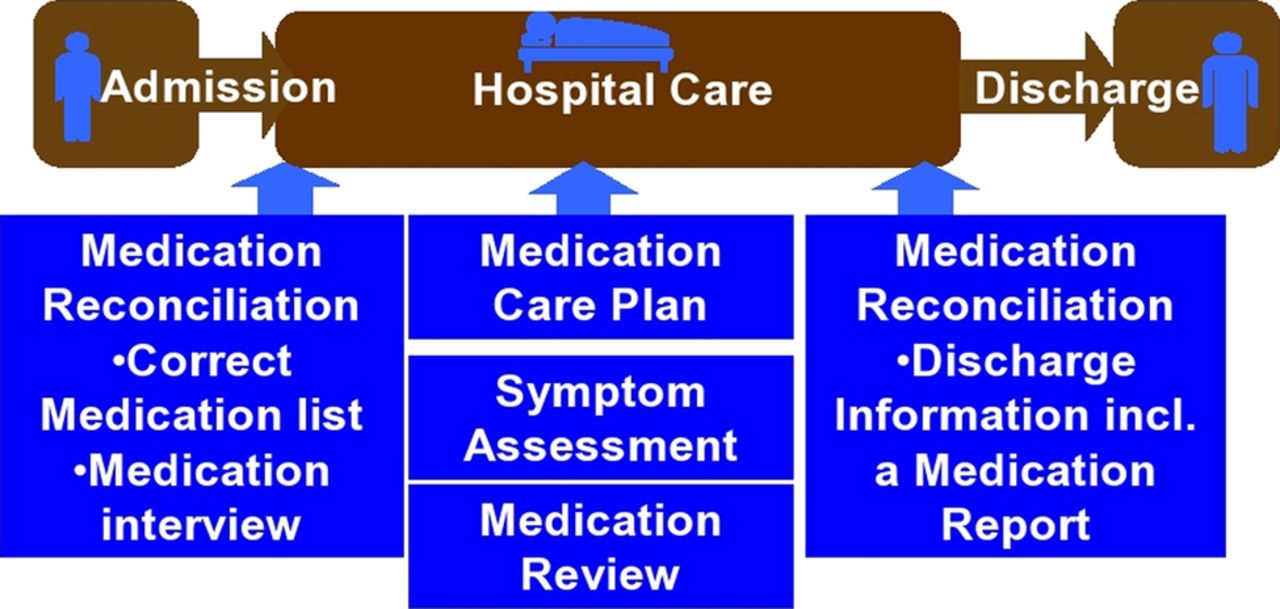
A systematic analysis of potential problems and limitations during the standard patient medication care process was performed in 1999. This followed admission, hospital stay and post discharge. We focused initially on the potential problems to assess their frequency and clinical significance. We also began to improve the structure and process for each of the three stages (admission, hospital stay and post discharge) to improve patient and healthcare outcomes. For each part, specific tools, checklists and responsibilities were developed and subsequently tested. The final structured model is team based and consists of systematic medication reconciliation, medication review, and oral and written communication, as described in figure 1 and table 1. The clinical pharmacist was the catalyst for improvement in the patient care team but each member had their specific responsibilities, and the physician was responsible for changes in prescribing. Each part of the model was developed, introduced into the care team and researched stepwise in cooperation with the key teams: pharmacy, medicine and nursing, in hospital and primary care. The project was based on internal medicine wards at Skåne University Hospital, Lund and Landskrona Hospital, Sweden.
The Lund Integrated Medicines Management model: activities performed in the hospital wards, responsible professional groups and tools for performing the activities
{kind=link}
The Lund Integrated Medicines Management model.
We used descriptive studies to investigate problems, comparative controlled studies to investigate improvements, and blinded evaluators for studies on errors, consequences and clinical significance. Where possible we used validated tools; if not, we developed and validated new tools. The study size was based on power calculations where applicable. We analysed results using descriptive and comparative statistics, trend, regression and survival analysis, intention to treat and per protocol analysis, and also probabilistic decision tree models for health economic evaluations. The number of included patients in each of the studies ranged from <100 to almost 4000.
Results
Nineteen scientific publications and manuscripts have been produced from the development, and also formed the basis for four PhD and more than 30 MSc theses. The model has been shown to improve the process of care—that is, it identifies and solves DRPs, reduces medication reconciliation errors and improves medication appropriateness. A summary of the benefits in the admission and hospital care process is presented in table 2 and in the discharge process in table 3. For each comparison, there was significant improvement (at least at the p<0.05 level).
Activities on admission and during hospital stay: summary of potential process benefits studied
Activities at discharge: summary of potential process benefits studied
The model also improved clinical outcome. Healthcare contacts and hospital readmissions due to medication errors were reduced by at least 50%13 ,16 but total readmissions were not affected.14 It also saved time, at least 2–3 h per patient, for physicians and nurses in hospitals, in primary and community care.17 The model also generated cost savings of €370, for each intervention cost of €42 and gained utility of 0.005.18 The probability that the intervention would be cost effective at a zero willingness to pay for a quality adjusted life year gain was 98%. Finally, physicians and nurses were very satisfied with the process and the pharmacist contribution.10 ,11 ,17 The model has been adapted to primary care medication review by pharmacists, and a randomised controlled study showed a decrease in potential inappropriate medication among the elderly.19
Discussion
For more than a decade, the Lund Integrated Medicines Management (LIMM) model has been developed and researched, and its benefit in the process and in some outcomes has been established using high quality methods and design for a team approach. During this period, several hundred pharmacists, physicians and nurses have been involved. Although the pharmacist is the catalyst and the lead professional in getting the process running, the roles of the physicians and nurses are fundamental for success. The model is transferable to similar healthcare systems, and outcomes can be guaranteed with the use of the tools, checklists and other support systems developed using LIMM process indicators and standards.
A recent Cochrane review concluded that it is uncertain whether medication review reduces mortality or hospital readmissions, but medication review seems to reduce emergency department contacts.1 However, the cost effectiveness of this intervention is not known, and due to the uncertainty of the estimates of mortality and readmissions and the short follow-up, important treatment effects may have been overlooked. The Cochrane review also states that medication review should preferably be undertaken in the context of clinical trials and that high quality trials with a longer follow-up are needed before medication review should be implemented.1
In our work, we have not had the opportunity of performing high quality trials called for by the Cochrane review. Our team approach with routines, responsibilities and trust have been designed over several months to be effective and safe. It is therefore not possible to randomise a patient to a control group. A team based randomised study can only be performed in clusters, and we have not had the financial or organisational power to perform such a study. This is a limitation in the evidence base for the model. However, to our knowledge, there are no high quality studies on team based model interventions in healthcare where real patient outcomes have been studied. Interrupted time series have been suggested as a way to analyse outcomes. This is however problematic when the number of events (outcomes) in each cell is very low. Mortality and hospital readmissions due to DRPs are such outcomes.13 ,14
The focus of this paper has been on the process of drug therapy. According to Donobedian,7 the structure of care is also very important for quality and outcome. As part of the structure we need pharmaceuticals and diagnostic tools with a high level of evidence. We also need educated and trained pharmacists, physicians and nurses. With this in mind, several courses have been developed at Lund University for students and practitioners. The LIMM model has had a large impact on pharmacist education with a full scale MSc pharmacy programme. Here the LIMM model is the educational platform for training pharmacotherapy, communication, clinical skills, etc.20 The model has also received several national awards, including best innovation in Swedish healthcare, the gold scalpel. In southern Sweden, each hospital has employed a number of additional clinical pharmacists, paid by the local authorities, to perform medication reviews according to the LIMM model. Very recently there was an amendment to the Swedish constitution and also a national patient safety agreement that healthcare professionals must perform medication review and medication reconciliation during care transitions, and there have been economic incentives for this. This is expected to have a large impact on the need for clinical pharmacists, which is good for both patients and the pharmacy profession.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; not externally peer reviewed.