Article Text

Abstract
Objectives We aimed at identifying drug-related problems in pain therapy and assessed the effect of medication management by pharmacists in routine care.
Methods We performed a cohort study consisting of a control (no pharmaceutical service) and a medication management group receiving pharmaceutical services including recommendations to physicians. We defined pharmacotherapeutic and administrative drug-related problems in pain therapy and analysed patient charts to assess the outcomes. Active participants in the study were not involved in study assessment. Outcomes were the number of patients and the number of analgesic prescriptions with drug-related problems.
Results We analysed 414 medication records (controls: 208, medication management: 206). Our intervention had no influence on the number of patients with drug-related problems following analgesic prescriptions (control: 166/208, 80% vs medication management: 155/206, 75%, p=0.266). In 98 control group patients (47%), we found at least four drug-related problems. This fraction was smaller in the medication management group, with 66 patients (32%; p=0.002). The number of analgesic prescriptions leading to drug-related problems decreased from controls with 381/627 (61%) to 308/654 (47%) in the medication management group (p<0.001).
Conclusions Current pain therapy standards were not strictly adhered to in routine analgesic prescriptions for orthopaedic patients. The inclusion of pharmacists into the team successfully decreased drug-related problems. However, further interventions are required to achieve optimal effects.
- PAIN MANAGEMENT
- CLINICAL PHARMACY
- MEDICAL ERRORS
- PHARMACOTHERAPY
Statistics from Altmetric.com
Introduction
Nowadays, pharmacists in the ward and in the backup office engage in a broad range of quality-related and patient-related aspects of individualised therapy.1 ,2 The inclusion of pharmaceutical knowledge into an interdisciplinary team contributes to better clinical outcomes. Drug–drug interaction management,3 drug dosing in patients with renal insufficiency4 and special pharmaceutical issues such as incompatibilities5 are examples of areas in which successful interventions enhance quality improvement. Furthermore, pharmacists collaborate with physicians, nurses and other healthcare providers in order to achieve lower mortality rates and higher cost efficiency.6 ,7 Yet, pain therapy remains an area in which collaboration of pharmacists and physicians in an interdisciplinary team is rarely reported. Especially, intervention studies investigating the benefit of such collaborations are widely missing.
Severe pain strongly impairs the quality of life.8 Patients fear pain or face barriers to pain management while undergoing surgery in hospital.9 Therefore, analgesic therapy, one of the important pillars of pain management, should be of special concern in quality improvement strategies. The role of pharmacists has already been discussed with regard to particular areas of pain therapy such as opioid overprescribing.10 Positive effects of educational interventions that pharmacists delivered to patients with chronic pain have been reported.11 Moreover, in outpatients receiving palliative care, pharmacists have been shown to contribute to optimised pain therapy and symptom control.12 As previously reported,13 multidisciplinary pain management including interventions by pharmacists increases guideline adherence and even improves the patients’ individual pain situation. In summary, the literature has mainly dealt with chronic pain in patients with tumour so far.
Recently, nationwide guidelines have been published addressing, for example, perioperative acute pain management.14 These guidelines recommend best practices of pain therapy including pain assessment and evidence-based treatment in general and with a focus on surgical procedures. Although these guidelines give advice on how to handle practical aspects of pain therapy, their implementation has not been fully completed yet.15 This situation is associated with an elevated risk of drug-related problems. Therefore, we aimed at investigating whether drug-related problems occurred in orthopaedic patients in a hospital setting with routine prescriptions of analgesics (control group). We hypothesised that a comprehensive pharmaceutical service would influence the prevalence of drug-related problems in pain therapy (medication management group).
Materials and methods
Participants and setting
Patients on three orthopaedic wards with 49 beds at our university hospital were eligible for the study. In specific pain situations, physicians in the ward could request consultative examination by pain therapists or an acute pain service, a structured programme by pain nurses under supervision of pain therapists. An internal standard for pain therapy, however, did not exist at the time of this study.
Study design
We performed a cohort study consisting of a control (without pharmaceutical service) and a medication management group (with pharmaceutical service). We included patients who were hospitalised in the participating wards during the respective study periods. In both the groups, patients were included consecutively, only once and only during their first hospital stay within the study period. All control group patients were discharged before any pharmaceutical service was implemented. The first period (control group, 9 weeks) started in May 2010 and the second study period (medication management group, 10 weeks) in May 2011. The medication management group received comprehensive medication management provided by pharmacists. This structured service was prospectively planned and implemented in July 2010. Four pharmacists with several years of experience in clinical pharmacy provided this service. It was offered within routine care for all newly hospitalised patients and, additionally, once a week for all patients in the wards included. The pharmacists assessed the adequacy of the patients’ medication including parameters such as dosing, formulation and drug–drug interactions. On completing the medication management, pharmacists informed physicians about their recommendations (eg, modification of the medication profile or monitoring of laboratory data) in a written form.
Study assessment
We predefined drug-related problems with analgesic prescriptions (including co-analgesics). Active participants in the study were not involved in study assessment. Drug-related problems were defined as deviations from nationwide guidelines for pain therapy,14 from WHO standards,16 from the Summary of Product Characteristics, from drug information services17 and from the current literature about medication errors and their evaluation.18 ,19 We classified drug-related problems into pharmacotherapeutic or administrative problems. We analysed analgesic-related data gained from patient charts to assess therapy adequacy with respect to predefined drug-related problems. For the assessment of prevalence, we considered the prescription in the last version of the patient chart before discharge and analysed analgesics prescribed to patients during their hospital stay. Patients were not included in our study in those cases where their charts were not available. We analysed the data after the study periods had finished. This ensured that any influence the data evaluation might have had on the pharmacists participating in the study was excluded.
Outcomes and power calculation
We assessed the number of patients (primary outcome) and the number of analgesic prescriptions with at least one drug-related problem. The prevalence of those problems per prescription, per patient, in total, within predefined categories, and the number of prescribed analgesics were further aspects we recorded (secondary outcomes). According to the results of a previous study regarding tumour pain13 and pilot investigations in acute pain settings, we hypothesised that without medication management at least 50% of patients would be affected by at least one drug-related problem in pain categories. A decrease by at least 15% (as compared with the control group, ie, a rate of ≤35% in the medication management group) was considered clinically relevant. Assuming rates within the mentioned range, a double-sided test at a significance level of α=0.05 and a sample size of at least 167 patients will provide a power of 1-β=0.80. We presented data as median with the first and third quartile or as frequencies of the respective patients or prescriptions, as appropriate. Results were analysed by χ2 test or Mann–Whitney U test, as appropriate. Patient characteristics were analysed to ensure comparability of patient groups and to exclude potential result-modifying factors. In the analysis of secondary outcomes, we made no adjustment for multiple testing. A p value of <0.05 was considered significant. Calculations were conducted using SPSS (Statistical Package for the Social Science, V.20, IBM, USA).
Results
Altogether, 478 consecutive patients were hospitalised in the participating wards during the study periods. A medication profile was available for 414 of those patients, of which 208 patients were in the control and 206 in the medication management group. Patients were mainly hospitalised for surgical interventions (59% in controls vs 65% in the intervention group) or conservative orthopaedic treatment including pain therapy (41% vs 35%). Patient characteristics did not differ between the two groups (table 1). Participating physicians (n=21, including six senior physicians) were orthopaedics with a professional experience ranging from 1 to 37 years. Physicians prescribed a median of three analgesics (Q25/Q75:2/4) per patient, in both the control and the medication management group (n.s.). We analysed 627 analgesic prescriptions by physicians in the control group and 654 in the medication management group. Apart from WHO-II opioids, which were less frequently prescribed in the medication management group (p=0.002), prescription behaviour concerning other analgesics remained comparable in the two groups (table 2).
Patient characteristics
Prescribed analgesics, with 627 analgesics prescribed in the control group and 654 in the medication management group
Our medication management had no influence on the number of patients with at least one drug-related problem with analgesic prescriptions (controls: 166/208, 80% vs medication management: 155/206, 75%, p=0.266). In 98 (47%) of the control group patients we found at least four drug-related problems. This fraction decreased to 66 (32%; p=0.002) patients in the medication management group.
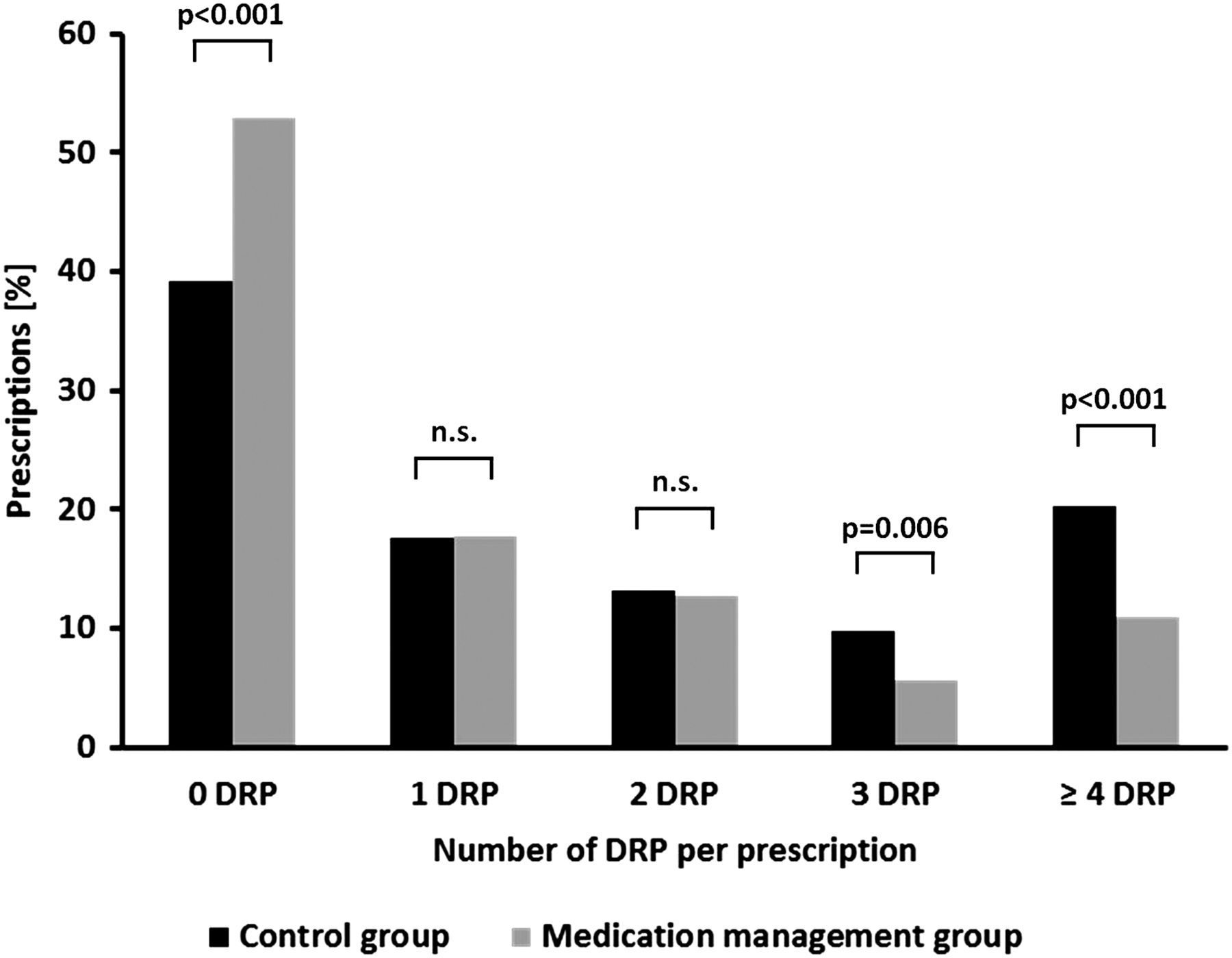
With 381/627 (61%), the number of analgesic prescriptions with at least one drug-related problem was lower in the control group than in the medication management group with 308/654 (47%; p<0.001). The rate of drug-related problems/prescription decreased from 1.77 by 31% to 1.22 (relative risk reduction (RRR); p<0.001), and notably, prescriptions with 3 and ≥4 drug-related problems decreased significantly (p=0.006 and p<0.001; figure 1).

{kind=link}
Distribution of prescriptions in relation to the number of drug-related problems (DRP) per prescription in the control group (black, total of 627 prescriptions) and in the medication management group (grey, total of 654 prescriptions).
Regarding pharmacotherapeutic drug-related problems, analgesics in problematic ‘pain cocktails’ and ‘opioids in inappropriate combination’ were significantly less frequently prescribed in the medication management group as compared with controls (p=0.005 and p=0.041, table 3). Other subgroups in this area remained without statistically significant alteration. Among administrative drug-related problems, several subcategories such as incomplete information concerning single dose, dosage instruction (eg, dosing interval), daily dose and drug name or dosage form improved (each p<0.001).
Predefined categories of drug-related problems in pain therapy
Discussion
We found that, based on current pain standards, drug-related problems in analgesic prescriptions were alarmingly frequent, with 80% of orthopaedic patients being affected in controls. This indicates that strategies for quality improvement in this field are absolutely necessary. We prevented drug-related problems in pain therapy by involving pharmacists in the multidisciplinary team.
Due to the interventions, prescriptions with drug-related problems moderately but significantly decreased from 61% to 47%. Mainly prescriptions with three and more drug-related problems declined, and prescriptions without any drug-related problem reached more than 50% in the medication management group. This is an important but not sufficient step to improve pain therapy. Especially patients suffering from a large number of drug-related problems benefitted from the medication management. However, the number of patients with at least one drug-related problem with analgesic prescriptions remained unaffected by our intervention. This indicates a need for a more frequent medication management.
Our once-a-week service addressed the individual patients’ pain medication rarely more than once during their hospital stays. Pain therapy should regularly be tailored to the individual pain situation. Hence, if pharmacists participate in pain therapy management, they should be involved in a daily ward round or patient chart analysis to reach an optimised benefit. Within daily service, pharmacists could give recommendations after any change of medication or in the clinical situation. They could check if their recommendations are put into practice and, if necessary, repeat these recommendations. Optimising the implementation as well as reducing communication and documentation problems should even improve the positive outcomes.
Our study was restricted to the assessment of drug-related problems (predefined standards) and did not assess the actual pain of patients. A multicentre study by Vallano et al20 reported that pain prevalence was higher in those patients in whom analgesic treatment did not adhere to guidelines. Therefore, the high prevalence of drug-related problems in our study indicates insufficient pain control in our patients. Thus, under the medication management, the prevalence of drug-related problems decreased respectably by an RRR of nearly one-third. Our results support the point of view that pharmacists play an important role in the interdisciplinary team by supporting physicians in a broad range of therapies.21
Physicians quite commonly prescribed analgesics in problematic ‘pain cocktails’, which frequently were combinations of dipyrone, tramadol and metoclopramide. Mainly because of their inconsistent quantitative composition and unclear stability, experts consider such combinations obsolete. Due to medication management, physicians prescribed ‘pain cocktails’ less frequently, with a decrease of 41%.
A further positive outcome might be that WHO-II opioids were prescribed less frequently in the medication management group.
Identified drug-related problems may result in avoidable adverse effects because analgesics are among the drugs with significant harm potential.22 Non-steroidal anti-inflammatory drugs (NSAID) in particular, possess increased end organ toxicity and may further reduce perioperatively reduced renal function. They also inhibit thrombocyte function, leading to an increased risk of bleeding. Especially in the elderly, as in our patient group, NSAIDs pose a particular risk of causing gastric ulcer.23 Opioids, on the contrary, can lead to adverse events that go along with a reduced quality of life. Constipation and vomiting, in particular, are among the most frequent adverse events requiring pharmacotherapy with supportives such as laxatives or antiemetics.24 In this study, however, the medication management did not significantly improve supportive care. Thus, we identified this point as one of the key aspects for further interventions.
The high prevalence of drug-related problems, which was reduced due to the medication management, underlines the need to further involve pharmacists in interdisciplinary teams. Opioids were identified as a particular target of educational interventions.25 Inclusion of pharmacists and co-working with physicians have already been implemented in primary chronic pain management.26–29 However, apart from counselling healthcare providers, future pharmaceutical strategies should also address the patient directly.30
It is a special strength of this study that active participants in the study were not involved in study assessment. Thus, we excluded any influence of the involved pharmacists on the assessment of their interventions. This is in contrast to a former study13 in which the intervening investigators assessed their own effects. Moreover, we did not assess the prevalence of interventions addressed by pharmacists in this evaluation but the number of drug-related problems identified by an independent review of the patient charts. This way, we investigated whether drug-related problems were resolved and whether modifications of the medication management were actually put into practice.
Limitations
While analgesic overdosing was not a major problem in our study, analgesic underdosing and inadequate pain treatment might be a result of missing information about pain intensity. Pain and pain intensity were not routinely documented on the wards involved. As a consequence of these findings, documentation of pain intensity will be implemented and investigated in a further project. It should be taken into account that structured pain assessment influences pain therapy even in the control group without additional intervention and that, therefore, pain assessment itself is, in itself, an intervention within the total quality process of pain treatment.13
Even though we are not aware of any specific confounder or bias, we cannot completely exclude modifying factors due to the non-randomised study design. To minimise these effects, we chose the same study units in controls and in the medication management group in order to assess the same staff and to ensure verified comparability of the two patient groups. Additionally, we chose the same time of the year for the two study periods to avoid seasonal impact.
Conclusion
We identified pain in orthopaedic patients as an important field for quality improvement strategies in routine care. Pharmacists support analgesic prescribing practices by physicians in a collaborative manner considering administrative and pharmacotherapeutic drug-related problems. Our medication management once a week might be a pragmatic but successful instrument transferable to other settings with limited resources. However, intensified interventions (eg, with daily feedback to physicians) are required to achieve the full benefit for all patients.
Key messages
-
What is already known on this subject?
-
Including pharmacists in the interdisciplinary team contributes to better outcomes in many medical fields.
-
Pain therapy is a typical field for interdisciplinary teamwork. Yet, pharmacists are not regularly involved in routine pain management so far.
-
Recently, guidelines for perioperative acute pain management have been published but their implementation in routine practice remains unclear.
-
Studies investigating the contribution of pharmacists to improving guideline adherence in perioperative pain therapy and to solving drug-related problems, caused by insufficient guideline adherence, are still missing.
-
What this study adds?
-
We found that drug-related problems in pain therapy were alarmingly frequent in routine care.
-
Involving pharmacists on a weekly basis contributes to a substantial improvement in following pain standards for orthopaedic patients.
Acknowledgments
We would like to thank all participating pharmacists, physicians and nurses on the ward for their kind support. We also thank PD Dr Astrid Bertsche and Sabine Budnick for proofreading our manuscript.
References
Footnotes
-
Funding Susanne Schiek was co-financed by the Saxony Chamber of Pharmacist.
-
Competing interests None.
-
Ethical approval The Ethics Committee at the Medical Faculty of Leipzig University approved the study (approval no. 384-11-12122011).
-
Provenance and peer review Not commissioned; externally peer reviewed.