Article Text

Abstract
Objectives Physicochemical incompatibilities between intravenous drugs are a recurrent problem in hospital settings. Having observed a drug precipitation during Y-site administration in our intensive care units, we undertook an investigation to find out its cause.
Methods We conducted a literature search on the injectable drugs involved in the observed precipitates and undertook laboratory physicochemical incompatibility testing of potentially incompatible drug combinations not reported in the literature.
Results Among the drugs tested, only furosemide with midazolam or with monobasic potassium phosphate was physically incompatible. The pH-dependent solubility of furosemide was the origin of the observed incompatibilities.
Conclusions Monobasic potassium phosphate is not compatible with furosemide in the concentration range used in our intensive care unit and should not be administered together in the same intravenous line. Other drug formulations buffered to a low pH should not be administered with furosemide solutions either.
- Stability and Incompatibility
- Intensive & Critical Care
- Y-Site Injection
- Furosemide
- Potassium Phosphate
Statistics from Altmetric.com
Introduction
Physicochemical incompatibilities between intravenous drugs are a recurrent problem in intensive care units (ICUs),1 ,2 where most of the drugs are administered continuously. Thus, despite the use of multilumen catheters, several drugs flow together in the same line. Poorly documented (in)compatibilities involve, among others, intravenous monobasic potassium phosphate (KH2PO4)3 frequently used to supplement patients with hypophosphataemia or to rapidly compensate a hypercalcaemia.
Recently, significant white cloudy precipitates were observed in central intravenous catheters in our adult ICU. The patients concerned received four to eight drugs continuously in the same intravenous line (same lumen of the central venous catheter), including KH2PO4 (table 1). These patients also received furosemide, a drug solution known to be incompatible with many others due to its high pH.3
Drugs administered in the same intravenous line in six patients in the catheter of whom a white cloudy precipitate was observed.
The aim of this study was to identify the origin of these incompatibilities.
Methods
Literature search
A search for literature reports on incompatibilities between pairs of drugs administered simultaneously was performed.3–5
Visual assays
Visual assays were performed to assess the compatibility between two drugs either in the absence of published information (KH2PO4 with furosemide, heparin sodium, human insulin, midazolam, propofol or remifentanil) or when the literature provided controversial or incompatible results (furosemide with midazolam or magnesium sulfate and KH2PO4 with magnesium sulfate).
The tests were performed in transparent and colourless glass test tubes with a flat base. The concentrations and solvents chosen were the same as commonly used in our adult ICU (figure 1).
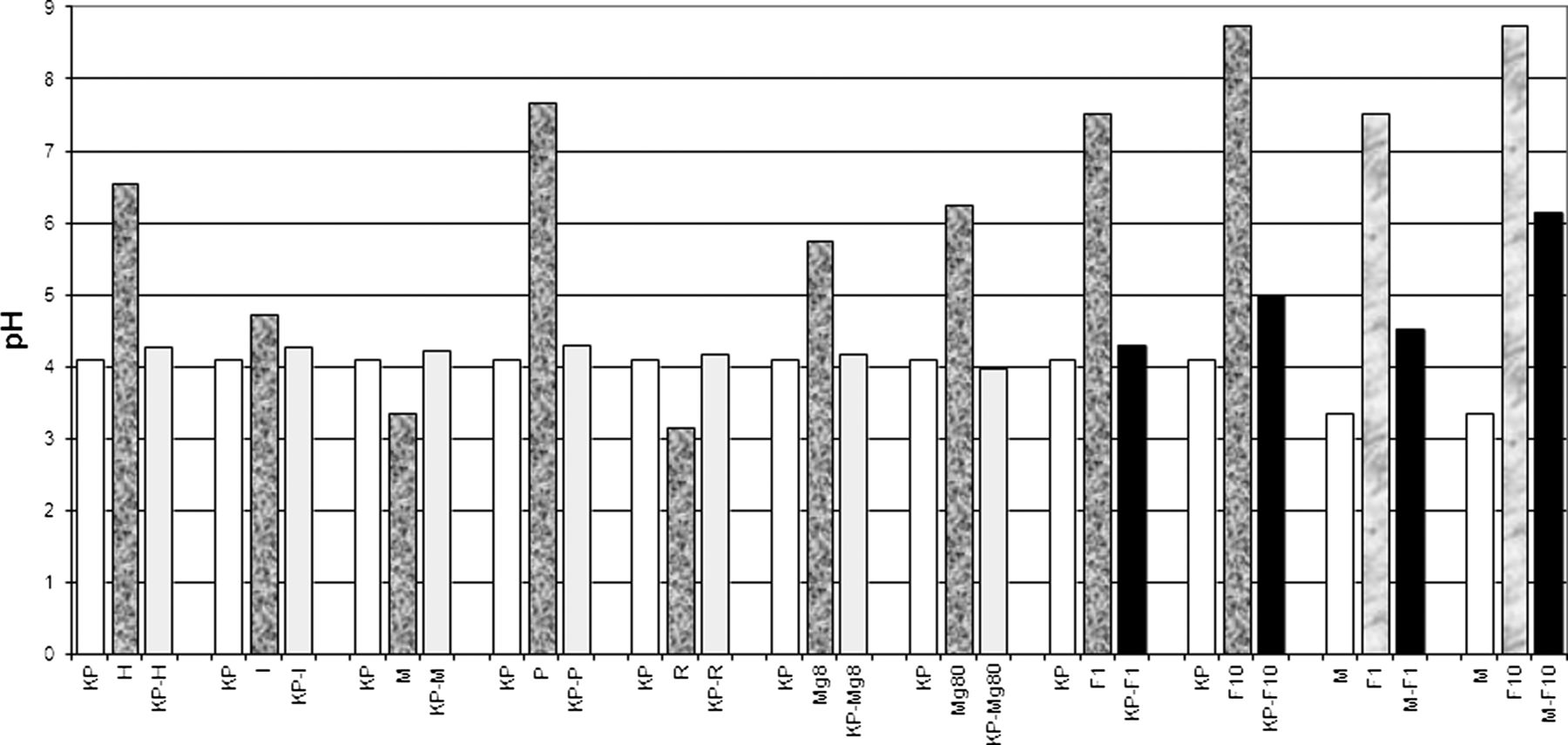
{kind=link}
pH values of single-drug solutions and their pairwise mixtures. For each mixture, the pH represented here is the mean of the pH values measured at 15 min, 30 min, 1 h and 2 h, for the 1:1 mixed test. The black bars correspond to the formation of a precipitate. Standard deviations were small (≤0.1) and are not shown. Key: (1) KP=monobasic potassium phosphate KH2PO4 (Potassium Phosphate B Braun 1 mmol/mL, 10 mL) undiluted (pH=4.10). (2) H=heparin sodium (Liquemine Roche 5000 UI/mL, 5 mL) 416.7 UI/mL in NS (NaCl 0.9%) (pH=6.55). (3) I=human insulin (Actrapid HM Novo Nordisk 100 UI/mL, 10 mL) 1 UI/mL in dextrose 5% (pH=4.73). (4) M=midazolam (Dormicum Roche 5 mg/mL, 3 mL) 1 mg/mL in dextrose 5% (pH=3.35). (5) P=propofol (Disoprivan PFS AstraZeneca 20 mg/mL, 50 mL) undiluted (pH=7.67). (6) R=remifentanil hydrochloride (Ultiva GSK 5 mg) 0.1 mg/mL in dextrose 5% (pH=3.14). (7) Mg8=magnesium sulfate (Magnesium Sulfate Bichsel 100 mg/mL, 10 mL) 8 mg/mL in NaCl 0.9% (pH=5.75). (8) Mg80=magnesium sulfate (Magnesium Sulfate Bichsel 100 mg/mL, 10 mL) 83.3 mg/mL in NaCl 0.9% (pH=6.24). (9) F1=furosemide sodium (Lasix Aventis Pharma 10 mg/mL, 2 mL) 1 mg/mL in NaCl 0.9% (pH=7.53). (10) F10=furosemide sodium (Lasix Aventis Pharma 10 mg/mL, 2 mL) undiluted (pH=8.74).
For each pair of drugs, four different tests were performed, namely: (A) 1 mL+1 mL, no mixing, (B) 1 mL+1 mL, mixing, (C) 1 mL+4 mL, mixing, (D) 4 mL+1 mL, mixing.
Duplicate combinations were prepared, with permutation of the addition order for the two combinations. The 1:1 ratio was chosen according to Allen et al.6 The 1:4 and 4:1 ratios were used to simulate cases where one of the two drugs is administered faster than the other and will thus reach higher concentrations at the tubing Y-site. The two drugs were mixed with a Mini Vortexer VWR for 5s. The 1:1 ratio test without mixing was performed to better simulate a Y-injection where mixing is not always immediate. Glass tubes were closed and maintained at room temperature for 24 h without light protection. Solutions were examined for any visible change after 6 min, 15 min, 30 min, 1 h, 2 h, 4 h and 24 h and the pH was measured after 15 min, 30 min, 1 h and 2 h. The tubes were inspected macroscopically, first against a white background to look for any colour appearance and then against a black background with polarised light to look for a precipitate, opacity or creaming of lipidic solutions.7 Drugs were considered compatible when no change was detectable within 24 h.
Determination of the solubility of furosemide as a function of pH
Among all checked drugs, furosemide is known to be a frequent source of incompatibilities.3 Due to its acidic properties, it must be solubilised in a slightly basic solution and is often incompatible with drugs soluble in slightly acidic solutions. We therefore determined the pH-dependent solubility of furosemide. Phosphate buffers (Na2HPO4.2H2O, Merck, Germany and citric acid, Hänseler AG, Switzerland) were prepared and adjusted at pH 2.00±0.05, 3.00±0.05, 4.00±0.05, 5.00±0.05, 6.00±0.05, 7.00±0.05 and 8.00±0.05; other buffers (Na2CO3, Merck, Germany and NaHCO3, Sigma-Aldrich, USA) were prepared for pH=9.00±0.05 and pH=10.00±0.05.8 About 600 mg of furosemide powder was added to 10.0 mL of each pH solution and agitated for 6 h for maximal dissolution. The solutions were then filtered with a 0.45 μm PVDF membrane filter (Acrodisc PALL) and their pH adjusted to 8.00±0.05 with NH3 17.5 or 3.5% or HCl 0.5 N (pH value close to that of Lasix solutions).
The concentration of furosemide in each solution was then measured by HPLC9: HPLC Waters 2695 Alliance Separations Module (Waters Corp, USA) driven with the Empower Software; Symmetry C18 Guard Column 3.9×20 mm (Waters) and Chromolith Performance RP-8e 100×4.6 mm, 2 μm (Merck, Deutschland) as stationary phase; 0.2 g KH2PO4 (Merck, Germany)+0.25 g cetrimide (FeF Chemicals A/S) in 70 mL water, pH adjusted to 7.0±0.05 with NH3 17.5% and addition of 30 mL propanol as mobile phase; flow rate of 1 mL/min; temperature of the column fixed at 30°C; injected volume of 100 μL for the pH 2, pH3 and pH4 solutions, and 50 μL for the other solutions; Waters 2996 photodiode array detector with a fixed length of wave of 238 nm as detector.
Results
Literature search
According to the literature, only the simultaneous administration (Y-injection) of furosemide and midazolam or magnesium sulfate5 ,10 is reported to have led to a precipitate, whereas data about the compatibility of magnesium sulfate with KH2PO44 ,5 are controversial. Besides, there is no information on the compatibility of KH2PO4 with furosemide, heparin sodium, human insulin, midazolam, propofol or remifentanil.
Visual assays
KH2PO4 and furosemide showed physical incompatibility, with the formation within a few minutes of a dense cloudy white precipitate. Concentration seemed to play a role, since the precipitate appeared more rapidly with the 10 mg/mL than with the 1 mg/mL furosemide solution. Besides, the mixing of midazolam with furosemide also led to a rapid precipitation, while the mixture of magnesium sulfate with KH2PO4 was visually compatible for 24 h, at least at the tested concentrations, as well as the mixture of KH2PO4 with the other tested drugs.
The results of pH measurements are represented in figure 1, showing a dramatic pH change between the mixture and one or both drug solution(s) in cases a precipitate was visible (ie, furosemide-midazolam and KH2PO4-furosemide). Three other mixtures, namely KH2PO4 with heparin sodium, magnesium sulfate or propofol, also showed a significant pH change, but without precipitation or emulsion break in the case of propofol lipid emulsion.
Determination of the solubility of furosemide as a function of pH
Our investigation showed as expected from the structure of furosemide that its solubility was indeed pH-dependent (practically insoluble at pH <6, 10 mg/mL at pH=7, 15 mg/mL at pH=8 and 35 mg/mL at pH=9 and 10).
Discussion
Of the pairs investigated, only two appeared to be incompatible, namely (A) midazolam and furosemide, already described in this way in the literature, and (b) KH2PO4 and furosemide. This latter incompatibility was unpublished and may explain the precipitates observed in the ICU patients’ catheters. For patient 3, midazolam may even have worsened the phenomenon, being also incompatible with furosemide.
Furosemide is an organic acid with a pKa of 3.9. The drug is much more soluble at neutral and basic pH values where its anionic form predominates. The solubility of furosemide is comparable with that of other sparingly soluble ionisable drugs presented by Avdeef11 and, in our study, the concentrations of furosemide measured at low pH (pH=2 and pH=6) were similar to those described by Beyers.12 Even if the nature of the buffer may be a significant factor in drug solubility,13 pH appears as the only critical factor in furosemide solubility.14 Lasix for injection, which has a high pH (8.90), will thus be incompatible with acidic solutions. In our case, addition of acidic solutions, either KH2PO4 1 mmol/mL (pH=4.10) or midazolam 1 mg/mL in dextrose 5% (pH=3.35) lowered the pH enough for part of the drug to precipitate.
According to literature, furosemide is indeed incompatible with acidic drug formulations (eg, ciprofloxacine (pH=3.9–4.5), milrinone (pH=3.2–4.0), gentamicin (pH=3.0–5.5), labetalol (pH=3.0–4.0), vinorelbine (pH=3.5) and gemcitabine (pH=2.7–3.3)) (3). In contrast, formulations with neutral or basic pH are compatible with furosemide (eg, tirofiban (pH=6.5), dexamethasone (pH=8.0–9.0), ceftazidime (pH=6.0–8.0)).3
The incompatibility between KH2PO4 and furosemide was added to the Table of Drug Incompatibilities we provide to the nursing staff at the ICU. Since KH2PO4 and furosemide are often administered continuously, the only way to avoid an incompatibility is to separate the two drugs in different lines. The use of an alternative phosphate salt yielding a higher pH (eg, sodium glycerophosphate, pH=7.4) could also be considered.
The other solutions producing an important shift in pH without formation of a precipitate indicate that the solubilities of heparin sodium, magnesium sulfate and propofol are not pH-dependent. Finally, the reported incompatibility of magnesium sulfate with potassium phosphate1 could not be reproduced in this study, possibly due to different concentrations or other factors. Under our conditions, no precipitate was apparent and this association was considered as compatible, in agreement with another report.2
Conclusion
KH2PO4 is not compatible with furosemide in the concentration ranges used in our ICU and should not be administered together in the same intravenous line. Other drug formulations buffered to a low pH should not be administered with furosemide solutions either.
Footnotes
-
Contributors This paper was reviewed and approved by all named authors, and each contributed significantly to the publication.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.