Article Text

Abstract
Objectives In 2013, the PharmaHelp device was introduced to daily patient care at the University Hospital of Heidelberg in order to improve process and staff safety and health. It is a semiautomated device located in a safety workbench for aseptic preparation with weight-and-visual-supported process check as well as radio-frequency identification of bags and vials.
Methods After qualification and a training period, several high-admixture-volume drugs were chosen stepwise to be prepared by the device. During a reporting period of 6 months, the number of processed production runs and produced bags were assessed as well as the productivity per hour of the device based on the processed admixing volume and time consumption for manual preprocessing and postprocessing steps.
Results Weight conformity tests of 246 processed bags in 11 admixing-volume ranges showed 99.19% with a deviation of <5%. Validation of the automated preparation process with 40 media fills showed no microbiological growth. Daily patient care production in the first 6 months led to a nearly similar weight accuracy and an average productivity of 22.5 preparations per running hour of the device at an average admixing volume of 39.6 mL, excluding manual preprocessing and postprocessing tasks. Time consumption for all manual steps was about 76 min per run.
Conclusions The automated admixing process of the device showed remarkable effectivity and a satisfying accuracy, but the manual preprocessing and postprocessing steps are time consuming, which is associated with the local environment, and has to be reorganised.
- PHARMACY MANAGEMENT (PERSONNEL)
Statistics from Altmetric.com
Introduction
At the Heidelberg University Hospital, approximately 550 000 patients per year are treated in about 50 medical departments. In addition to those departments, the hospital pharmacy takes care for the National Cancer Center, 1 of 12 high performing cancer centres in Germany, which is supported by the German Cancer Foundation. The pharmacy prepares about 78 000 individualised aseptic preparations per year for intravenous administration to patients with cancer. This contributes to patient safety and quality of treatment by management of accuracy as well as chemical stability and microbiological purity as recently described.1 The preparation takes place in laminar airflow workbenches on a volumetric basis. Two technicians work at one workbench with regular rotations, performing in-process crosschecks. To provide a service without greater delays, chemotherapy is prepared 1 day in advance on a patient-individualised basis whenever stability and cost aspects allow.
To prepare for future challenges, we considered to introduce an automated preparation approach. The first experiences in automated antineoplastic drug preparation have been published in 19902 and various experiences with fully automated robots followed more than one decade later,3 ,4 but approaches and local conditions that influence use and output of the device are different. In addition, there is already evidence that robotic devices are able to produce very low contamination levels,5 and therefore, might be capable of enhancing staff safety.6
After scanning the market for available possibilities, consultations with the manufacturer and careful consideration of all aspects, the decision was to choose the semiautomated option PharmaHelp, Fresenius Kabi, Bad Homburg (figure 1).

The semiautomated PharmaHelp device.
Functionality
The device is incorporated in a safety workbench (width 1.94 m, distributor Telstar), and can be installed in every Good Manufacturing Practice class B or C cleanroom area. Holder, connecting pinches, syringe carousel and robot head occupy about three-quarters of the workbench space. One-quarter is available for aseptic preparation procedures, and is separated by a slidable dividing window. A touchscreen monitor is placed outside on the right-hand side of the workbench, functioning as controlling unit of the robot. Part of the product package was also two PCs, two scales (accuracy limit 0.2 mg), one of them attached to a camera for preprocessing and postprocessing of the materials and the holders with integrated RFID (radio-frequency identification) chips for infusion bags and vials. In addition, a starting package of syringes and venting needles, which contain an air filter (PharmaVent) and admixing needles (PharmaNeedle) for withdrawal and admixture of drugs, was provided. The included software for control of production steps and record of audit trail had been placed on a virtual server of our hospital with support of the company at the time of installation of the device. It has the capacity to prepare up to 16 bags in one run. There is also the possibility to withdraw a defined volume of carrier solution from the bag and to transfer it in a waste bag before admixing of the drug. This reduces the possible number of preparations to 15 because in this case one slot is occupied by the waste bag. On recommendation of the manufacturer, it is possible to work with up to six different drugs during one run. Withdrawal and admixing steps are fully automated, which provides improved staff safety compared with manual compounding. The device is also capable of processing leftover vials from previous runs. Up to now, it is not possible to prepare elastomeric pumps and bolus syringes. The extensive software-supported safety check functionalities (release process, weight-based preparation and visual vial label checks) allow that preprocessing and postprocessing for recent and future runs can be performed simultaneously while a production run is in place.
Preprocessing and postprocessing steps have to be done manually, preferably in another workbench as well as reconstitution of lyophilic drug vials, which can be used afterwards in the device.
After transfer via interface or manual introduction of prescriptions to the PharmaHelp software and release by a second person, orders can be selected for the run. All materials are displayed and have to be picked manually, and their lot numbers to be registered in the software. Actual lot numbers, which are on stock, can be introduced in advance, so that they will be offered by the system. Vials and infusion bags have to be associated manually to special holders that fit on the two scales, which are used for preprocessing and postprocessing as well as the pinches on the bar inside the workbench. Via the RFID chip in the bag and vial holders, the distinct infusion bag and drug vial is registered during the weighing step on the first scale, and identified during every following process step (robot head and second scale) of the device. After the weighing step, which can be processed either inside or outside a workbench, which is subject to where the scales are placed, vials have to be manually equipped with venting needles under aseptic conditions. The holders with bags and vials have to be connected to the bar of the device, syringes connected to the special PharmaNeedle and attached to the carousel inside the workbench. The automated preparation run is now ready to be started. The operator is now able to fulfil other tasks (eg, preprocessing and postprocessing) while the run is in place. After the run, the holders with the infusion bags have to be unloaded and weighed again to verify the correct addition of drug volume. The exact weight of admixing volume is calculated by using the density of the processed drug. After RFID verification and weight assessment of the preparation, the label is generated immediately. Which information the label should contain is subject to individual settings created by the user. Bags and vials are now to be removed from the holders; vials with leftovers stay at the holder, and can be selected at picking on one of the following runs with this drug. Waste disposal has to be performed manually. Final step is the release of the produced bags by the responsible pharmacist. An overview of described process steps is shown in figure 2.
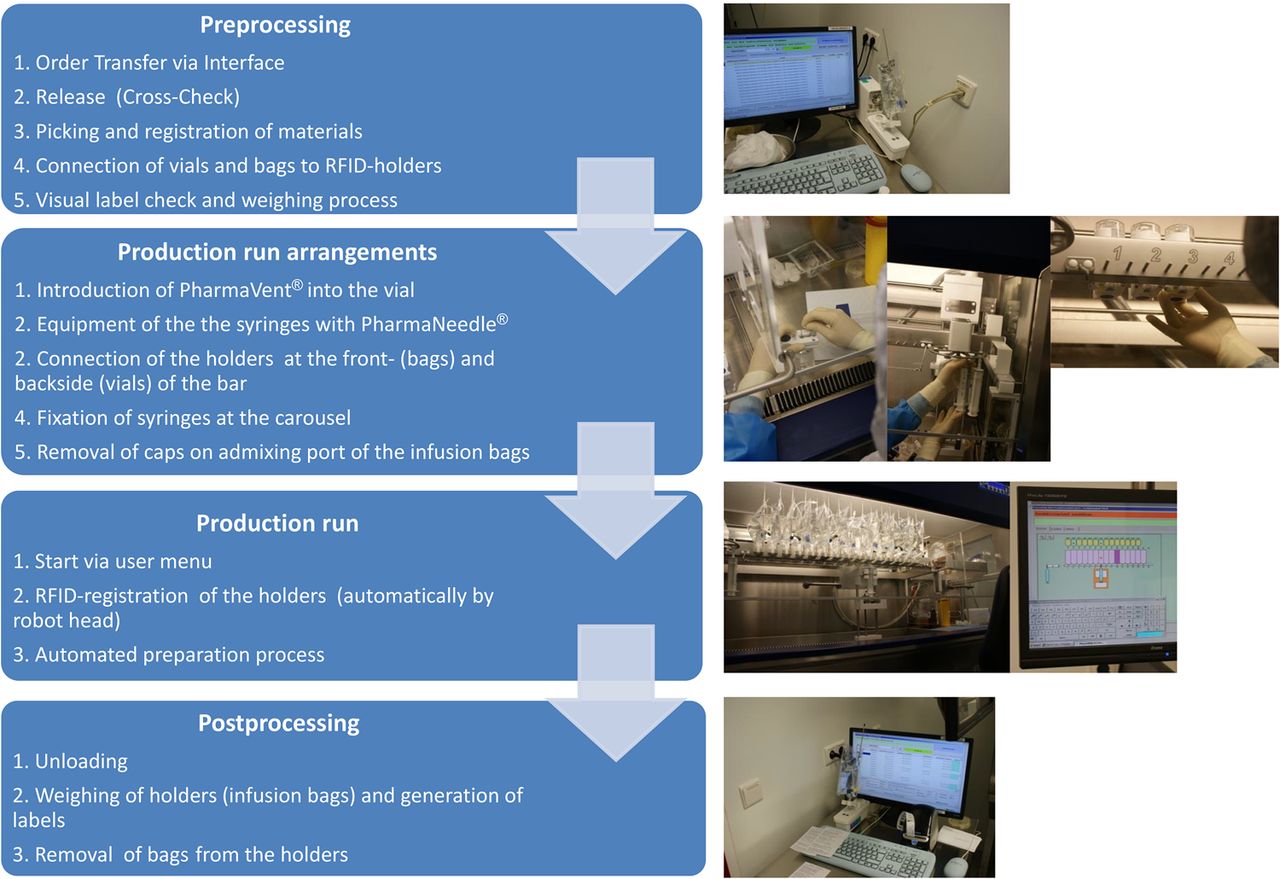
PharmaHelp process scheme. RFID, radio-frequency identification.
Materials and methods
The manufacturer has already provided substantial data for the performance of the device. These were data on weight conformity at different adding volume ranges, cross-contamination (analytical tests of prepared bags), work-environment contamination (wipe tests) and microbiological process validation (media fills).
During a 7-month on-site training and testing period, we generated data on weight conformity, a microbiological standard monitoring (contact and settle plates) and a microbiological validation of the preparation process by media fills. The project team consisted of a pharmacist, a technician and a practical examination student.
After the test period, we started to use the device in daily patient care, and evaluated extension of use, dosing accuracy, productivity parameters and further experiences.
Test on weight conformity
During a timeframe of 1 month, we prepared a total of 246 dummy preparations (sodium chloride 0.9% and dextrose 5%) with different amounts of admixing volumes (5–42 mL). Scales had been calibrated and certified by an external service provider (Mettler Toledo, Gießen) before start, and scales had been tared daily by using a standard weight.
Settle and contact plates
We performed four contact and four settle plate tests daily inside the workbench area for 14 consecutive working days. Settle plates (CASO-Agar European Pharmacopoeia (Ph Eur); Oxoid, Wesel, Germany) were placed inside the workbench on different critical points, contact plate tests (CASO-Agar with neutralizer Ph Eur) were performed alternately on different surfaces of workbench and device (working surfaces, holding bar, robot head, syringe carousel, window surface). Cleaning of workbench and device surfaces took place daily in the morning (Ethanol 70%, Alkopharm) and after finishing work with an alkaline, disinfectant detergent (Septolit 1%, Ecolab). Plates were incubated for 7 days at room temperature and 7 days at 32°C according to the recommendations of Ph Eur.
Media fills
In addition, we performed five media fills daily on eight consecutive working days with the PharmaHelp device. An amount of 40 mL saline chloride 0.9% was withdrawn from the infusion bags (Freeflex 50 mL, Fresenius Kabi, Bad Homburg) followed by the addition of 90 mL of Sojapeptone-Caseinpeptone Solution (Ph Eur). Bags were incubated for 7 days at room temperature and 7 days at 32°C.
Daily patient care practice
During a reporting period of 6 months, the number of processed production runs and produced bags as well as accuracy of results was assessed by analysing the data collected by the software of the device. In addition, after the reporting period, we conducted a manual assessment of total time consumption for preprocessing and postprocessing steps. Therefore, we selected two production runs, which were processed on two different days by two different staff members. Detailed descriptions of materials, process steps and calculation of results are demonstrated in table 1. These were compared with the results of an assessment of a manual volumetric-based preparation of one bag (cisplatin, admixing volume 48 mL) in a safety workbench by two staff members. Here, the following steps were monitored: label check, picking, disinfection and transfer of materials into the workbench, gloving, handling of materials inside the workbench, preparation using a spike for withdrawal and a cannula for admixing, labelling and final check. All steps were multiplied by 15 to reach a result for 15 bags except for picking (multiplier 5) and gloving (multiplier 2) to simulate the reality of campaign-based preparation.
Assessment of total time consumption for preprocessing and postprocessing tasks and automated production from two processed runs (run 1 and run 2)
Results
Qualification: weight conformity
Weight conformity tests of 246 preparations in 11 admixing-volume ranges showed 99.19% of processed bags with a deviation of <5%. One preparation showed a deviation of 5.37%. Two preparations (0.81%) showed a deviation of >5.37%, both around 20%. These deviations might be due to handling errors during the weighing process, but we were not able to finally specify the reason.
Qualification: microbiological monitoring
After two positive results of one colony found on settle plates (day 2 and day 8), the completion of some tasks was shifted to another workbench (eg, attachment of lines to infusion bags), which led to no more positive results. All contact plate tests were free of microbiological contamination.
None of the examined media fills showed any turbidities, and were evaluated as free of contamination.
Statistical data from daily patient care
Between June 2013 and January 2014, we produced 3672 preparations (273 runs). On average, 13 preparations per run were processed. Five runs were excluded from the evaluation because of incompletion due to technical problems. Depending on the daily number of prescriptions, we performed between two and six runs per 8 h working day in the PharmaHelp device.
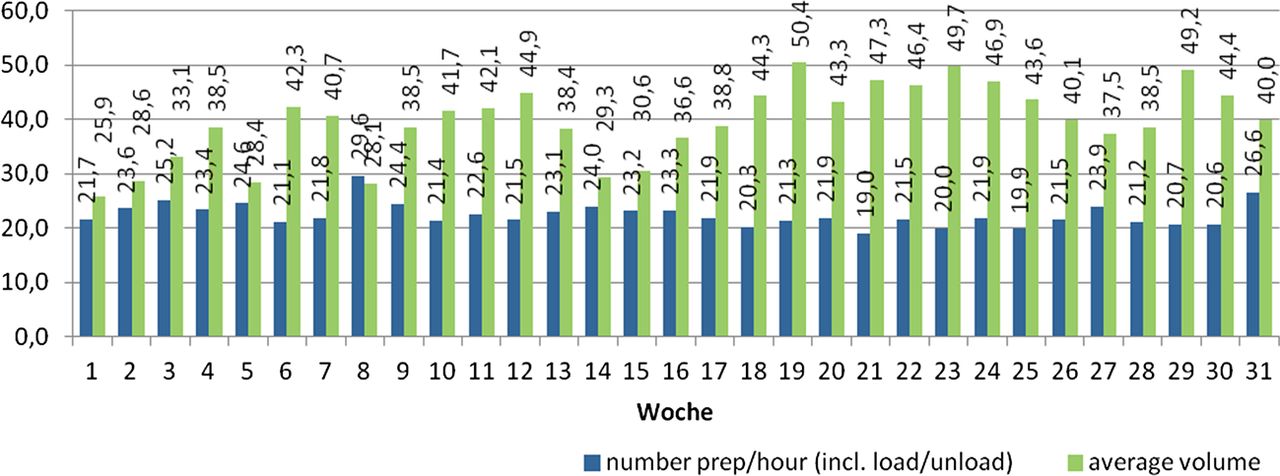
The number of preparations of used drugs within the reporting period and their average admixing volume are shown in figure 3. Whereas 85.74% of all preparations showed a weight deviation of <1% from the target dose, 13.91% of preparations displayed a deviation between 1% and 5%, and 0.35% of preparations were out of our locally defined acceptable range of >5%. Weekly productivity (including loading and unloading of the device, but excluding all other preprocessing and postprocessing steps) differed according to admixing volume (figure 4), and was 22.5 (19–29.6) preparations per hour on average at an average admixing volume of 39.6 mL (25.9–50.4) per preparation in the reporting period. These productivities neither include the time for preparation of the workbench, infusion bags and vials, weighing processes, final labelling and packaging nor took any withdrawals of carrier solutions placed during these runs.

Number of preparations per drug (blue bar) and corresponding average admixing volume (red bar).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Weekly productivity per running hour of the device in relation to average admixing volume.
The assessment of total processing time is presented in table 1. For the manual steps, we assessed 1:14 h (run 1) and 1:19 h (run 2). Automated production process took 0:23 h (run 1) and 0:34 h (run 2). As it is possible to perform the manual preprocessing and postprocessing steps while the automated production run of another batch takes place, these are the total processing times of the staff. In comparison, the assessment of manual volumetric-based preparation of one bag of cisplatin and extrapolation to 15 bags as described above led to a result of 1:06 h. The production steps (withdrawal from the vial and admixture into the bag) alone took a great part of this time (0:27 h).
Discussion
The PharmaHelp device provides the opportunity to automate the process that has the highest risk of pharmacy staff exposure—the admixing process of antineoplastic drugs. The device being incorporated in a normal safety workbench allowed an easy installation into our existing infrastructure. The concentration of the robotic automation only on the preparation step keeps the technical complexity of the device simple. This has resulted in very few down times. User support offered by the manufacturer has been satisfying. We never had to wait for more than 1.5 days in case of any problems; most issues were solved instantly via remote maintenance.
Handling was quite easy to learn and train due to a simple software menu and structure of the device. Accuracy of results was satisfactory. An interface to our prescription software offers a one-click-transfer of selected productions.
The automated production run itself showed a satisfactory productivity right from the start of patient care. The best output is reached by selecting runs with only one drug because in this case, the device has to pick only one syringe, and is able to do several admixings with one withdrawal of drug limited by the volume size of the syringe (60 mL). Greater deviations were mostly associated with particular drugs like paclitaxel, ifosfamide, irinotecan, cyclophosphamide and etoposide phosphate. This was mostly due to aspiration of air, which was caused by several reasons: for drugs with high viscosity (eg, paclitaxel), settings have to be adapted concerning the speed of withdrawal. Very oily drugs should reach room temperature (eg, rest vials from the fridge) before use. If powders or lyophilisates are reconstituted, it is necessary to use cannulas or spikes with a very small diameter; otherwise, the hole in the rubber leads to air aspiration during withdrawal, and deviations due to underfilling may occur. Vials with very soft rubber stoppers that close insufficiently after penetration with the cannula may lose droplets because they are hanging upside down in the device. We only experienced that once with one particular drug (cetuximab).
Whereas fully automated robots are able to perform several prepreparation and after-preparation processes as well as automatic waste disposal, with the PharmaHelp, these steps have to be handled manually. We were able to show with our assessment that all manual tasks, even if they are performed by experienced staff, are still very time consuming, and are the productivity-determining steps. This is highly dependent on staff's training level on the device and the kind of process organisation, especially influenced by the infrastructure, which in our case is difficult due to unfavourable room space. Some preparing tasks like the attachment of venting needles to the vials have to be shifted to workbenches located in other rooms, and materials have to be collected from other areas. We aim to improve this situation with the possibility of moving the device to another room to have a workbench close or opposite to the PharmaHelp bench to be able to plan preprocessing workflows fluidly. As the time consumption assessed for preprocessing and postprocessing steps is mostly independent from the processed admixing volumes, we were reassured to choose preparations of high admixing volumes for the device because in the manual production, these take considerably longer, and are associated with a higher physical burden. Seger et al7 showed that mean drug preparation time increased by 47% on using a fully automated robotic approach compared with manual compounding. Even if we also assessed a slightly shorter time consumption for a comparable manual process (about 66 min), we see several advantages in using a robotic device as already described recently:8 The assessed time consumption refers to one person working at the device, whereas the manual volumetric-based preparation is strictly bound to two persons for safety reasons (number of materials in the working area, in process-cross-checks). Staff can take care of preprocessing and postprocessing steps for recent and future runs while the production run is being performed automatically. The automated production process prevents upper limb disorders9 and reduces staff exposure. In addition, as we have been working on a volumetric base ever since, the device is able to improve patient safety by reducing the potential for human errors through weight and camera-based verification steps of correct dosing and a complete process audit trail. At the moment, we are awaiting an update of the vial label check software for the camera which provides a very complex user menu and is difficult to handle. In addition to that, recognition process of labels, sometimes, works quite slowly because the camera needs an exact positioning of the label.
So far, only one spillage inside the workbench was experienced due to an oblique position of the bag’s admixing port, which led to a violation of the port wall by the cannula and injection of the drug into the workbench space. We evaluated this event as an error caused by insufficient attention of the operator during loading of the device.
The high workload and the aggressive cleaning procedures led to a certain abrasion of bag and vial holders. These were replaced, and the currently used generation of the holders is much more convenient to handle. Cleaning process does not differ significantly from that in normal workbenches except for the holders which add to these efforts. Because of the device, staff still has to handle potentially contaminated parts like used holders and the task of connecting the venting needles; the plan is to prove safety by conducting a wipe test study in 2015 where contamination levels on surfaces of the device, the holders and the workbench should be assessed.
Concerning work ergonomics, some new questions have been raised, which are due to the different body heights of the staff members. The bar on which the holders have to be connected is fixed inside the workbench, and therefore, small and tall people are sometimes facing physical burdens (muscle tensions) if they work a whole week on the device. Therefore, we adapted the working schedules to provide a better rotation, which led to no more problems.
Conclusion
We reached our first goal of introducing the device to daily patient care and reaching acceptable productivity. Next steps will be to add reconstituted drugs, the improvement of environmental working conditions and the software for run-independent preprocessing, which will offer the opportunity to register and weigh materials in advance without knowing which particular preparations will be produced. With these optimisations, we are confident to reach significant improvements in productivity and in reducing preprocessing time by up to one-third. Another perspective might be to prepare elastomeric pumps and perfusor syringes for the device; we have already received signs from the manufacturer for future possibilities.
The authors have no conflicts to declare and take full responsibility for the content of this publication. The authors did not receive any external support in writing the manuscript nor did they receive financial compensation for authoring the manuscript.
What this paper adds
What is already known on this subject?
Several automated and semiautomated systems have been introduced for the compounding of individualised antineoplastic intravenous solutions over the past few years.
Before the start of daily patient care with the semiautomated compounding robot PharmaHelp, this device had not been introduced inside a safety workbench in any German or European hospital pharmacy so far.
The knowledge of advantages, disadvantages and challenges in using these automated ways has to be improved.
What this study adds?
Information about functionality, accuracy, productivity and staff safety of this particular device based on own collection of data and practical experience.
Challenges concerning implementation, workflow and handling of the device as well as future perspectives of improvement.
Acknowledgments
The authors would like to thank Dr Lenka Taylor for her support in finalising the manuscript.
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.