Article Text

Abstract
Objective To investigate the overall probability of error in preparing and administering intravenous medicines; to identify at which stage of the process an error is most likely to occur; and to determine the impact of error correction on the error probability.
Design Systematic review and random-effects Bayesian conditional independence modelling.
Methods Medline and EMBASE were searched for studies on intravenous medicines. The error rates of each stage were extracted. These, expert estimates, and error rates from generic tasks, were used in a Bayesian conditional independence model to find error ‘hot-spots.’ The main outcome measure was the probability of at least one error occurring during intravenous therapy.
Results Nine published studies were identified for inclusion in the systematic review and meta-analysis. The overall probability of making at least one error in intravenous therapy was 0.73 (95% credible interval (CrI) 0.54 to 0.90). If error-checking was introduced at each stage of the process, the overall rate fell to 0.22 (95% CrI 0.14 to 0.31). Errors were most likely in the reconstitution step. Removing the reconstitution step by providing preprepared injections would reduce the overall error rate to 0.17 (95% CrI 0.09 to 0.27).
Conclusions Intravenous therapy is complex and error-prone. Error-checking at each stage could reduce the error probability. The use of preprepared injections may help by eliminating errors in the reconstitution of drug and diluent. However, it will be important to ensure that benefits are not outweighed by practical disadvantages such as an increase in selection errors.
- Medication error
- intravenous injections
- systematic review
Statistics from Altmetric.com
Introduction
Errors that occur in the prescribing and giving of medicines are common and important,1–5 with an observed overall error rate ranging from 3 to 45%.6–10 Intravenous therapy is complex, error-prone and potentially dangerous,11–15 especially in children.16 17
Causes of error
The preparation and administration of intravenous medicines have many stages, which represent multiple opportunities for error. Errors include: omission errors, failing to give the medication at all; selection errors, where the wrong drug or diluent is selected; and reconstitution errors, where dosage or concentration, for example, is wrong. If strategies to reduce risk are to be effectively targeted, it is necessary to identify the stages where errors are most likely. We do not consider here the second important component, namely the harm that may arise if the error occurs.
Our aims were: (1) to characterise the stages of the process of the preparation and administration of intravenous medications; (2) to determine the overall error probability in intravenous therapy using data from existing literature; (3) to identify the stages in intravenous therapy where there was greatest risk of error and which may be amenable to improvement; and (4) to determine the impact of error correction on the overall error probability.
Methods
Task analysis
A physician, pharmacist and epidemiologist analysed intravenous drug therapy in order to partition the process into its component parts. Using prior knowledge and the observation of the process in practice, we identified 12 main stages, and 26 substages in the preparation and administration of intravenous therapy.
Literature review
We carried out a systematic review of Medline and EMBASE (1990 to August 2006) to identify prospective studies reporting error rates in intravenous therapy. The search was carried out without language restrictions using a combination of text words and search terms, including (‘error,’ ‘mistake,’ ‘medical-error’ or ‘medication-error’) and (‘intravenous,’ ‘infusions-intravenous’ or ‘injections-intravenous’). Articles that cited or were cited by the included studies were also screened to identify any further relevant studies. Additionally, reference lists from important reviews and personal files were scrutinised.
Studies were included if they reported the incidence of errors in the preparation and administration of intravenous medicines and a detailed analysis of errors at different stages. Case reports were excluded.
Data extraction
We extracted data from each study to assign the error probability to each of the stages or substages of intravenous therapy. To provide other estimates, especially where no experimental data existed, we assigned literature values for human error rates for generic tasks such as ‘errors in simple arithmetic with self-checking’ to each substage. The generic human error rate is the rate experimentally established for human errors when they are categorised according to the scheme proposed by Kirwan.18 One investigator (REF) with expert knowledge of the process also estimated the likely a priori probabilities of error (priors) occurring at each substage (online appendix 1).
Statistical methods
We performed random-effects meta-analyses of the log odds of errors using the data available from each study at each substage to estimate a pooled odds of errors for that substage. Odds were converted back to give a pooled estimate of error probabilities. We then used the estimated pooled error probabilities at each substage to estimate the error probability for that stage. The model was fitted in a Bayesian framework in WinBUGS.19 Figure 1 shows the structure of the fitted Bayesian model. The Bayesian model allowed us to incorporate not only the variability observed in the data but also estimates of error rates from other sources into the analysis using prior distributions. Our prior distributions were derived by mixing expert opinion with generic human error probability at each substage to form a ‘mixture prior’ in 60:40 ratio (expert opinion: generic human error) (online appendix 2). Under a Bayesian framework, the informative mixture priors contribute more weight where a small amount of data is present and less weight where more data are present. It also permitted us to estimate the error probabilities using only the informative mixture priors for substages where no data were observed (ie, not collected in the primary studies).
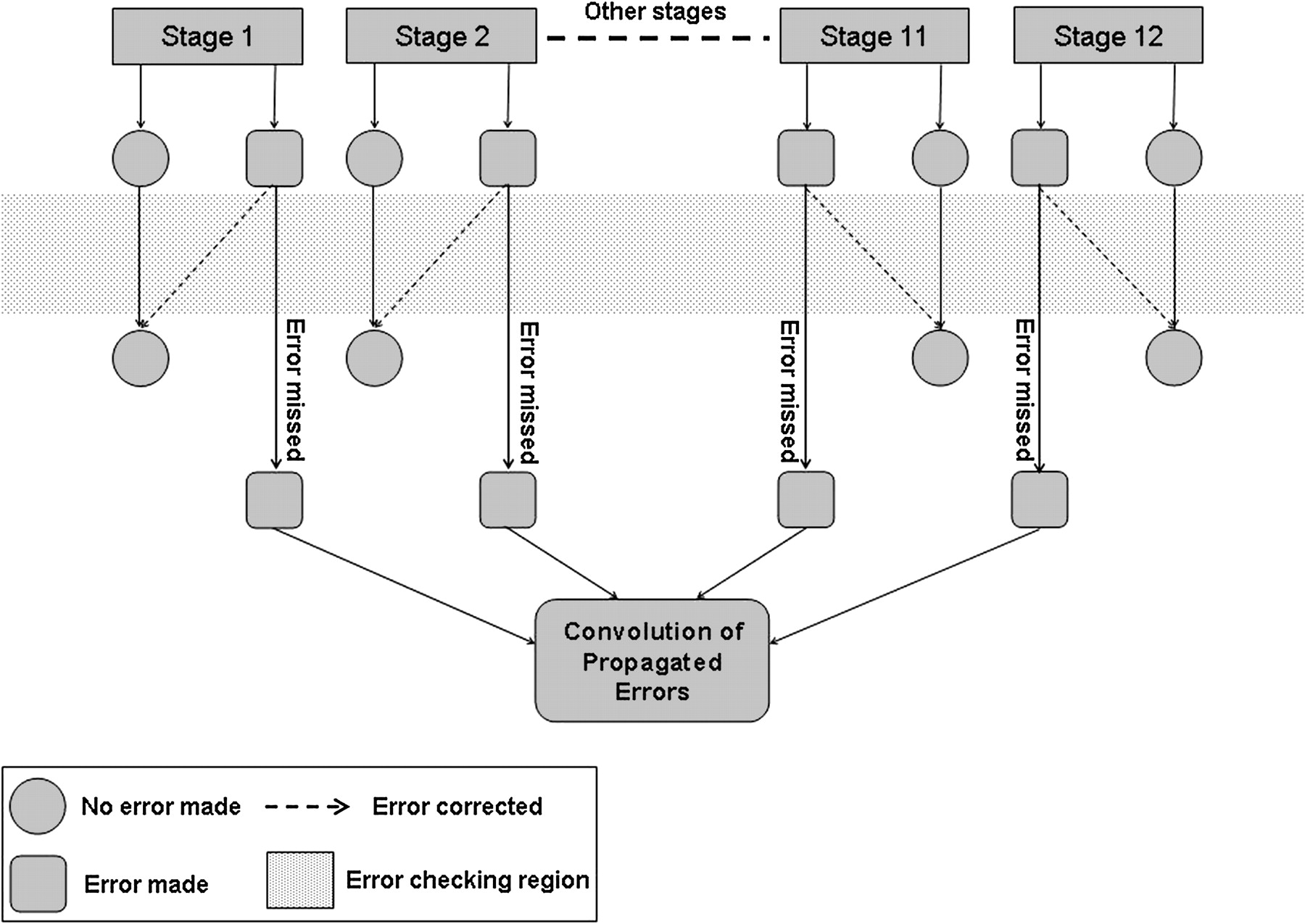
Illustration of structure of fitted Bayesian model when error checking is introduced.
The error probability at each substage was assumed to be conditionally independent of the occurrence of any errors in other substages given the error probability in that stage. The error probability at each stage was also assumed to be independent of other stages. Consequently, substages of one stage were independent of those of other stages. The overall error probability in the injection process under these assumptions was the sum of the probabilities from all possible paths of errors happening. In our analyses, we calculated the overall error probability as the complement of the product of the probability of no errors at individual stages. For simplicity, we then collapsed this into having no error at all and having at least one error.
We examined the likely effect of error-checking at each stage of the intravenous process (grey, shaded area in figure 1), assuming that the probability of detecting and correcting an error was 0.7,20 and of allowing it to enter the next stage was 0.3. We also assumed that the error-checking process itself would not introduce any errors.
We also explored the likely effect of using preprepared injections by removing the reconstitution step in the model.
Results
The systematic review identified 10 studies reporting errors in the preparation and administration of intravenous medicines (figure 2).21–30 One study was excluded because although it provided data from various stages, it was impossible to extract discrete data of the error probability at different stages.23 All of the included studies were carried out in European hospitals, one of which was a children's hospital (online appendix 3). All of the studies used the disguised observation technique, in which intravenous therapy was observed by a researcher without it being revealed that the true intent of the project was to identify error. Figure 3 shows the 12 stages and 26 substages we identified and adapted for this analysis.
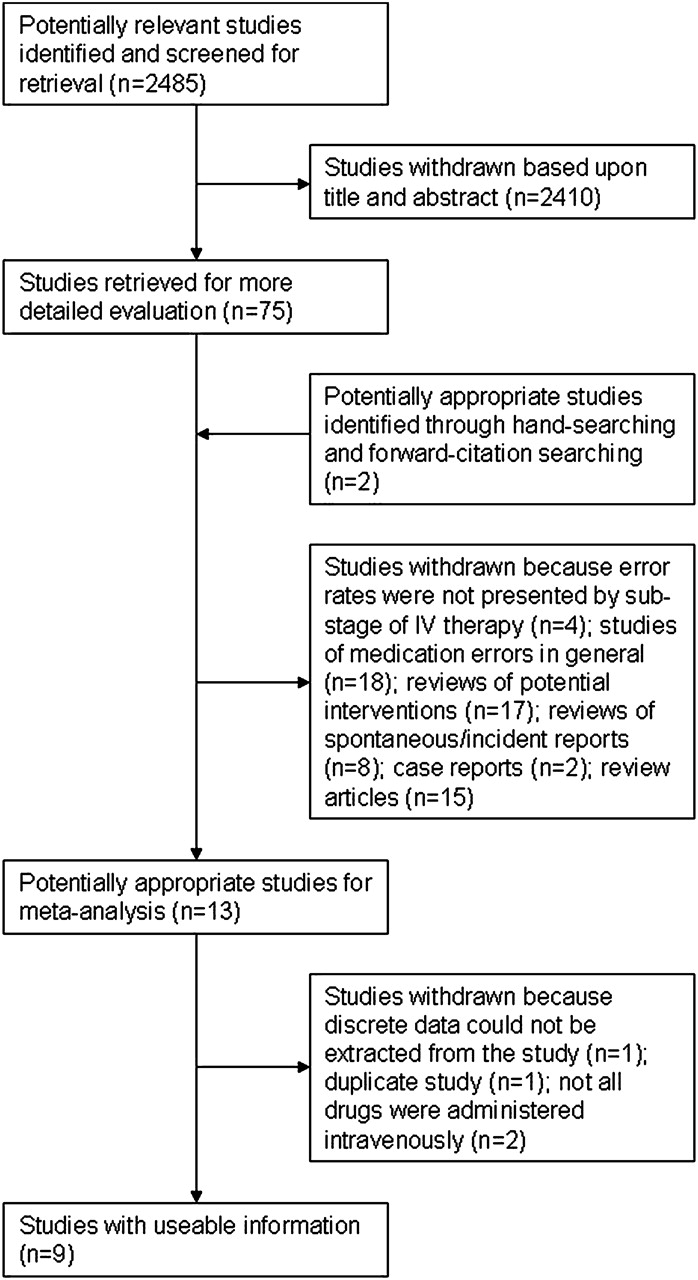
Flow chart of systematic review.

{kind=link}
{kind=link}
{kind=link}
Flow chart of intravenous therapy.
The available data were extracted from the nine studies (online appendix 3) and ascribed to appropriate substages of the intravenous process (table 1). Data were available from the literature for 10 of the 26 substages and for dose omission errors.
Number of errors by substage
We found that among the 12 stages, stage 3 (reconstitution of the drug and diluent) contributed the most errors P(error)=0.31 (95% CrI 0.12 to 0.50). Stage 4 (checking the patient's identity) contributed the least errors P(error)=0.001 (95% CrI 0.0001 to 0.01). The probability of an omission error (where the prepared drugs were not administered to the patient) was 0.03 (95% CrI 0.008 to 0.1). Table 2 shows the probabilities of errors (as percentages) at each stage.
Percentages of errors at each stage
The overall probability of not making any error at any stage during the 12 stages of intravenous therapy was 0.27 (95% CrI 0.10 to 0.46). The corresponding probability of making at least one error was 0.73 (95% CrI 0.54 to 0.90). If error-checking was introduced at each stage, then on the assumption of a 70% chance of detecting and correcting an error, the probability of making at least one error was reduced to 0.22 (95% CrI 0.14 to 0.31) (table 3).
Percentages of errors/no error occurring
We also conducted a sensitivity analysis to examine the effect of reducing and increasing the weight given to the generic human error in the mixture priors. Altering the weight did not significantly affect the overall error probability (online appendix 2).
Certain errors could be avoided if preprepared syringes were used. We assumed that this would remove stages 2 and 3 in the model because the diluent would no longer be required, and substages 1A and 1B would be a one-step process. Under these assumptions, the error probability without checking fell from 0.73 to 0.58 (95% CrI 0.35 to 0.83), eliminating about 21% of the errors. Overall error probability with error-checking fell from 0.22 to 0.17 (95% CrI 0.09 to 0.27), eliminating 23% of the errors.
Discussion
We found that the probability of making at least one error in the intravenous therapy process was high. Even with checking, one in five intravenous injections will have at least one error. With no checking, errors are substantially more likely. Our analysis indicated that two stages of intravenous therapy had the greatest error probability: the reconstitution of the drug and diluent; and the administration of the drug.
Errors in the making up and administration of intravenous medicines occur because of slips (or lapses) and mistakes such as dose calculation errors, selection of the wrong drug or diluent or the omission of a stage in the process. Poor training,31 32 poor labelling of ampoules, multiple ampoules of different medicines stored in the same area, insufficient staffing levels, distractions and fatigue contribute to the high risk of error.11
Several strategies have been suggested to reduce the occurrence of error, such as decreasing the number of steps involved in a process, improved training of staff33 and stocking only ampoules of one strength to prevent selection errors. The use of preprepared syringes or sealed systems that require minimal manipulation before use has also been suggested27; our results support this view. This may reduce the risk involved in the preparation of the drug and diluents. The reduced time spent in the preparation of the drug may also allow for a greater amount of time with patients. However, this strategy may increase costs, and there are issues relating to increased storage space requirements. This could also result in an increased risk of selection error owing to an increased number of preprepared phials of different drug doses and may make dosing less flexible.
Future research
Future studies that include the potential seriousness of error at each stage within the model could identify stages where there is both a high error probability and a greater severity of error and allow these ‘hot-spots’ of errors to be targeted. However, any change in the process of intravenous therapy will need to be tested in practice to ensure that reduction in errors of one type does not lead to an increase in other errors.
Limitations
Our analysis was primarily a statistical modelling exercise to examine the error probability within a complex process and has some limitations. Failure mode effects analysis (FMEA) is an effective process for identifying errors within a system. Several studies have focused specifically on intravenous medicines,34–36 but as such studies did not provide discrete probabilities of error for each substage, they could not be used in our Bayesian meta-analysis.
We analysed intravenous therapy in 12 stages, although other similar analyses are possible.37 A high degree of heterogeneity was observed between studies at each substage. Understanding the reasons for this heterogeneity would help inform the choice of probability for a specific context, but at the moment there is insufficient information to do this. Although the issue of medical error is a global one, the data were extracted from studies carried out in three different countries. While the processes and procedures have many common features, it is possible that conditions, temperament, training and other factors lead to systematic differences in error rates between different countries, and we have not accounted for these. We did not include errors that may occur in the prescription and transcription of doctors' orders. Research has suggested that errors in these stages are also frequent.38–40 Errors may occur in determining the correct drug and dose for the patient, particularly in the paediatric setting, where there is a lack of standardised dosing.41 Finally, we did not assess the impact of smart-pump technologies, which have been shown to aid in the detection of errors but not a reduction in their severity.42
There are very few experimental or observational studies of intravenous drug administration. Consequently, we have used information from other sources: an expert, whose views may not always be representative of the views of others; and a set of very broadly specified error rates derived from experiment and published for use in a different context. The sensitivity analysis (online appendix 2) showed that the results were robust in the face of different admixtures of priors. While the pathophysiology of error43 is understood and transferable from one general circumstance to another, the same may not be true for the very specific circumstances of operations in preparing an intravenous injection.
One further important question is the extent to which errors occur independently. Factors such as fatigue, inexperience and haste are known generally to increase error rates, and they might be expected to increase in the error rate for each stage. However, that would still leave open the question of whether the chance of an error at some later stage were dependent on the occurrence of an error at an earlier stage. Future experimental studies might examine this question.
Conclusions
Intravenous therapy is a complex process with multiple steps and multiple opportunities for error. We have shown how Bayesian statistical models can identify error ‘hot-spots’: steps in the process where error is most likely to occur. In our model, we identified the reconstitution of the drug and diluent, and the administration of the drug as the potential ‘hot-spots’ for error in intravenous therapy. The use of Bayesian analysis here, although complex, is more flexible than simple analyses, given that no data were available for half of the stages, because it enables us to make use of a broader body of evidence and judgement. Reducing the number of steps in the process and targeting interventions to specific ‘hot-spots’ should improve patient safety.
References
Footnotes
Funding SEM was supported by the Antidote Trust Fund of Sandwell and West Birmingham Hospitals NHS Trust.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.