Article Text

Abstract
Context Traditional manual/dictated discharge summaries are inaccurate, inconsistent and untimely. Computer-enabled discharge communications may improve information transfer by providing a standardised document that immediately links acute and community healthcare providers.
Objective To conduct a systematic review evaluating the efficacy of computer-enabled discharge communication compared with traditional communication for patients discharged from acute care hospitals.
Data sources MEDLINE, EMBASE, Cochrane CENTRAL Register of Controlled Trials and MEDLINE In-Process. Keywords from three themes were combined: discharge communication, electronic/online/web-based and controlled interventional studies.
Study selection Study types included: clinical trials, quasiexperimental studies with concurrent controls and controlled before–after studies. Interventions included: (1) automatic population of a discharge document by computer database(s); (2) transmission of discharge information via computer technology; or (3) computer technology providing a ‘platform’ for dynamic discharge communication. Controls included: no intervention or traditional manual/dictated discharge summaries. Primary outcomes included: mortality, readmission and adverse events/near misses. Secondary outcomes included: timeliness, accuracy, quality/completeness and physician/patient satisfaction.
Data extraction Description of interventions and study outcomes were extracted by two independent reviewers.
Results 12 unique studies were identified: eight randomised controlled trials and four quasi-experimental studies. Pooling/meta-analysis was not possible, given the heterogeneity of measures and outcomes reported. The primary outcomes of mortality and readmission were inconsistently reported. There was no significant difference in mortality, and one study reported reduced long-term readmission. Intervention groups experienced reductions in perceived medical errors/adverse events, and improvements in timeliness and physician/patient satisfaction.
Conclusions Computer-enabled discharge communications appear beneficial with respect to a number of important secondary outcomes. Primary outcomes of mortality and readmission are less commonly reported in this literature and require further study.
- Effectiveness
- evidence-based medicine
- hand-off
- information technology
- patient safety
Statistics from Altmetric.com
Introduction
Computer-enabled discharge summaries have been introduced in recent years in response to the well-documented problems faced by traditional handwritten and dictated summaries.1 2 Concerns about inadequate and incorrect content, lack of standardised structure and untimely information transfer are the most commonly cited.
Despite their growing popularity, there has been no comprehensive systematic review examining the efficacy of these new computerised systems. In 2007, Kripalani and colleagues2 investigated the prevalence of discharge communication deficits and looked broadly at all types of interventions that target those deficits. Of the 18 interventions identified, 16 of these were implemented prior to 2000; very few involved significant contributions of databases to construct the discharge summary, and none used the internet to transmit information. Much of the literature cited in a second review from 2007 included uncontrolled studies and some that were not peer-reviewed.3
This systematic review was carried out, therefore, in response to a significant gap in the literature. The objective was to evaluate the efficacy of computer-enabled discharge communication interventions for patients discharged from acute care hospitals.
Methods
Search strategy
A search of the literature was initially done on 15 March 2008, with the most recent updated on 1 November 2010 using MEDLINE, EMBASE, the Cochrane CENTRAL Register of Controlled Trials, and MEDLINE In-Process and Other Non-Index. The Cochrane Database of Systematic Reviews was searched to identify existing systematic reviews. We applied a detailed search strategy combining terms/keywords from the following three themes: (1) Discharge Communication; (2) Electronic/Online/Web-based communication; and (3) Controlled Interventional Studies.
For theme 3, the study design search filter described by Egger et al4 was amended to include both randomised clinical trials and other prospective interventional studies with control groups (ie, quasiexperimental studies with concurrent controls or controlled before–after studies). The initial search strategy was developed for use in MEDLINE, but was adapted for use in other databases. We considered both adult and paediatric populations, as well as studies in all languages. Hand searching of reference lists was also performed. The full search strategy is available from the authors on request.
Study selection
Titles and abstracts of all studies retrieved from the search were reviewed independently by two investigators (SMM, JP). Studies that were obviously unrelated and studies containing non-primary data were excluded in this first step. A full text review was then independently conducted by the same two reviewers for studies that were retained to determine if they met the inclusion criteria outlined below. Agreement among reviewers was quantified using κ statistics.
Inclusion and exclusion criteria
Interventions that focused on computer-enabled discharge communication, specifically for patients discharged from acute care to community care, were included. Also considered were computer-enabled discharge communications available directly to the patient. In order to be judged a ‘computer-enabled discharge communication,’ the intervention had to contain one or more of the following features: (1) automatic population of the discharge document by computer database(s); (2) transmission of discharge information via computer technology (eg, text message, email, or World Wide Web/internet); or (3) computer technology providing a platform for dynamic bidirectional discharge communication to occur between parties. Studies had to include a comparison group that received either no intervention or a traditional handwritten/dictated discharge summary. Studies included were therefore clinical trials, quasiexperimental studies with concurrent controls or controlled before–after studies.
Primary outcomes of interest were (postdischarge) mortality, readmission/emergency department visits and adverse events (including adverse drug events). Secondary outcomes included timeliness (time to complete, time to receive or time to read), accuracy of discharge information, quality/completeness and physician/patient satisfaction (including patient understanding of medical condition). Study-specific definitions for the various outcomes were compared and contrasted to determine the appropriateness of combining results across studies.
Studies with no comparison group were excluded, as were those without primary data, those with no reported outcomes and those not meeting our definition of a computer-enabled discharge communication (eg, non-electronic transmission, manually created documents or simple word processing). Additional exclusions applied to tele-health interventions that did not specifically relay discharge communication and to web-portals that contained only non-patient specific information (eg, only clinical practice guidelines, education materials, drug prescriptions and cost information, or referral information).
Data extraction and quality assessment
The data were independently extracted by two authors (SMM, JP) and entered directly into data tables. Differences in data-extraction decisions were resolved through discussion and review of source documents. Study quality for identified randomised controlled trials (RCTs) was assessed using criteria described by Jadad et al.5 Allocation concealment was also assessed, although this study quality criterion is not part of the Jadad score. For non-RCTs, the inferior study design was considered to be the main indicator of evidence quality.
Data synthesis
We compiled a detailed description of the selected studies with tabular presentation of the study design, intervention, outcomes of interest, results and study quality. A statistical met-analysis was planned a priori but was not performed, owing to the heterogeneity of measures across studies.
Results
The search identified 4415 articles that were initially assessed by review of titles and abstracts. Forty-nine of these were included for full text review. One additional study was identified through hand-searching of references, and another four identified on an updated verification search. A total of 12 studies published between 1992 and 2009 were considered unique and appropriate for final inclusion (figure 1). Study publications by Afilalo et al6, Lang et al,7 Callen et al8 9 and Graumlich et al10 11 reported data collected from common studies (and are therefore grouped in the tables below).
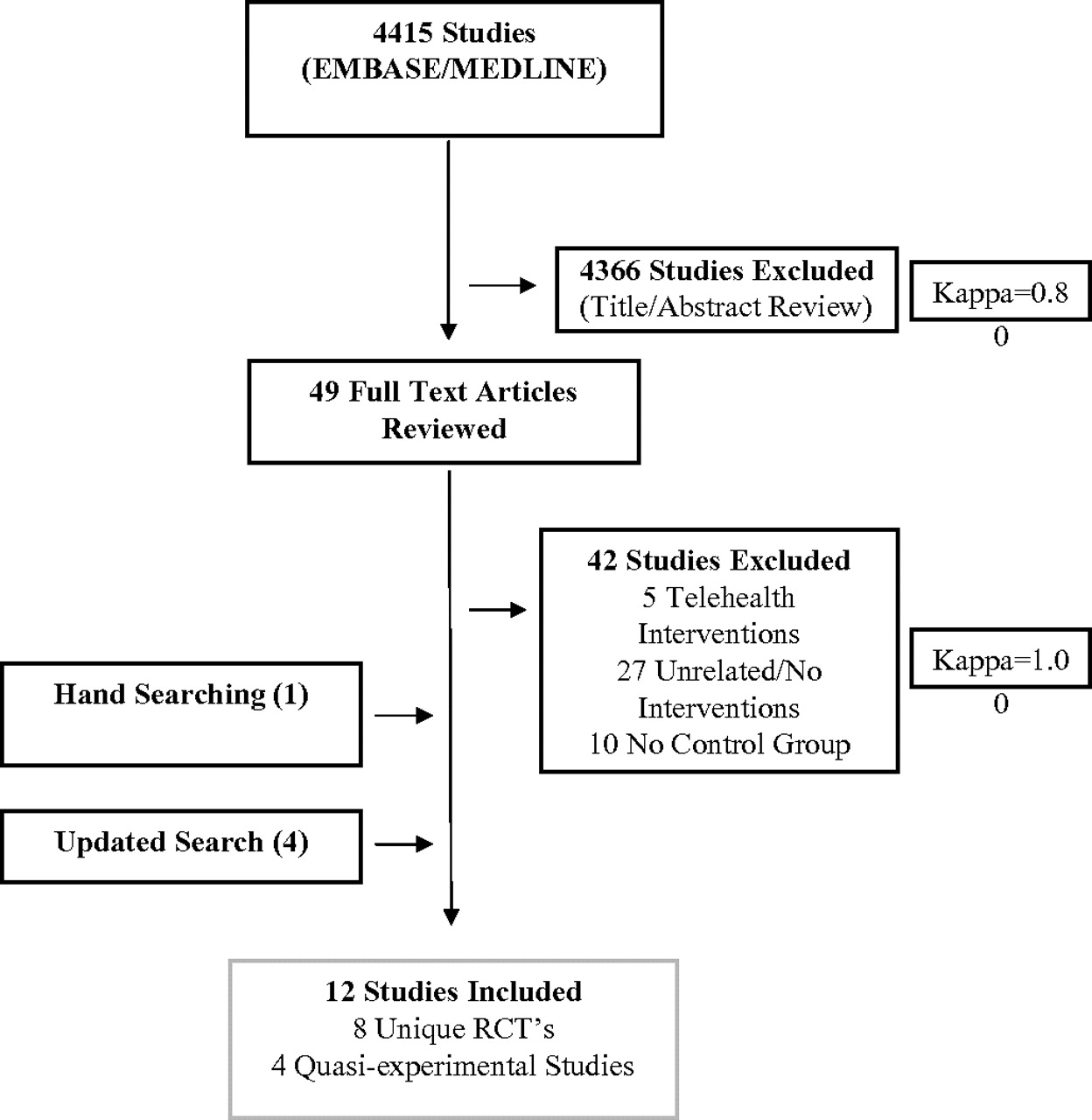
{kind=link}
Selection process for study inclusion into systematic review.
Description of studies and interventions
Eight RCTs and four quasiexperimental studies were identified (among the latter: 1 prospective cohort study with concurrent controls, and 3 before–after studies). In total, seven interventions employed computer database(s) to automatically populate the discharge document.8–14 Four studies explicitly stated that computer technology was used to transmit discharge information via text messaging, email or the world wide web.6 7 13 15 Two studies were classified as a computer technology providing a platform for dynamic discharge communication (including a web-based call center).16 17 One intervention combined all three features.18 Descriptions of each intervention are provided in table 1.
Characteristics of studies included in review by study design
Study quality
Each RCT was assigned a Jadad score5 of 3 or 4 out of 5, which is indicative of moderate study quality. Each appropriately described the procedure of randomisation as well as withdrawals/dropouts. No study explicitly performed double blinding. Allocation was concealed in all studies, except for perhaps two studies, where this methodological element was unclear. Table 2 provides a summary of study quality.
Study quality criteria that constitute the Jadad study quality score
Primary outcomes: mortality, readmission/ED visits, adverse events
Studies were quite variable with respect to outcomes reported (table 3). Only four studies reported on primary outcomes: three reported on both readmission and mortality,10 13 16 one reported on readmission only,6 7 and two reported on actual or primary care physician (PCP) perceived reductions in adverse events/near misses.13 14 No significant differences in mortality were reported between groups at 30 days, 6 months or 12 months.10 13 16 Readmission/emergency department visits were similar between groups at 14 days, 28 days and 6 months,6 7 and were significantly lower in the intervention group at 12 months.16 O'Leary et al14 reported a significant reduction in PCP perceived preventable adverse events (40.7% vs 30.2%, p=0.02) and near misses (65.7% vs 52.9%, p=0.008) over 6 months following deployment of an electronic discharge summary. Graumlich et al10 employed a more rigorous process of determining number of adverse events developed by Forster et al21 22 and reported no differences between groups in adverse events over 1 month.
Description of study outcomes and corresponding results
Secondary outcomes: timeliness, accuracy, quality/completeness, satisfaction
The majority of studies reported on at least one secondary outcome. Surveys/questionnaires were the most common means of data collection.6 7 11 13–15 17–19
Timeliness
Of eight studies, five showed that intervention discharge summaries were generated significantly more efficiently than traditional summaries and were transmitted to the PCP more quickly.6 7 11–15 20 23 The majority of intervention summaries were available within 48 h, while the control summaries were received from 1 to 106 days postdischarge.12 15 20 One study reported that intervention summaries were prepared significantly more quickly and easily, and reduced the burden on workload,20 two reported no difference in time burden,11 13 and one found that physicians perceived electronic summaries to require more effort to complete. It was not possible to pool timeliness data because each study measured time in different units (hours/days (including mean of 0 days)/or as a proportion of discharge summaries generated by a specified time).
Accuracy, quality/completeness
Accuracy and quality/completeness of discharge summaries were assessed using study-specific rating scales or by the number/percentage of omitted data elements. Only two studies examined accuracy in relation to transcription errors and reported that intervention summaries were more accurate or contained a similar number of errors.8 9 15 Three of five studies assessing completeness demonstrated significant improvements in the intervention group, specifically with respect to legibility,6 7 comprehensiveness6 7 and brevity,20 and more frequently included information on diagnosis,20 medications,20 planned follow-up,14 20 tests pending14 and information provided to the patient.14 One study found no differences in discharge summary quality.13 Callen et al8 9 had mixed findings and noted that intervention summaries contained significantly more errors/omissions regarding discharge date, additional/other diagnoses, follow-up requirements and discharge medications. A small number of physicians were responsible for 76% of all errors/omissions reported in this study.
Satisfaction
Eight studies reported on either the satisfaction of the physician (PCP, residents) with the discharge intervention or of the patient/family.6 7 10 11 13 17 18 20 Among all populations studied, satisfaction with intervention summaries was similar to or greater than that with traditional summaries. Each study employed unique definitions for satisfaction and, with three exceptions,11 13 18 used non-standardised/custom questionnaires.
Primary care physicians reported that intervention summaries were very useful and more comprehensive,6 7 15 providing them with better knowledge of their patients' hospital visits6 7 and the ability to ultimately better manage their patients.6 7 PCPs also generated significantly more follow-up actions upon receiving these summaries.6 7 Outpatient physicians studied by Graumlich et al11 also reported better perceptions of discharge quality for intervention patients who were discharged using computer software. Furthermore, residents expressed preference for the intervention over traditional dictated summaries.13 20
Patient/family preference varied by specific intervention. Patients with access to web-based resources in addition to personalised online discharge information16 or with access to Baby CareLink (a tele-medicine initiative providing daily clinical reports)18 had significantly improved knowledge of disease and self-management techniques and were more satisfied with overall quality of care and the care environment. Graumlich et al11 reported that patients who were discharged using the intervention discharge software perceived greater discharge preparedness and similar satisfaction to the usual care group with respect to knowledge of discharge medications. In the study by Maslove et al,13 computer-enabled discharge documents were provided directly to the patient, although attendance at follow-up visits/appointments and CTM-3 satisfaction scores were similar to those of patients whose discharge summaries were dictated (and these dictations were not necessarily provided to the patient).
Meta-analysis and summary visualisation of results
A priori, our study protocol anticipated possible meta-analytical pooling of outcomes. This was, however, not possible, given the heterogeneity of measures and outcomes reported across studies. Table 4 provides a semiquantitative summary of our review's findings. While no one study reports on all outcomes of interest, the body of literature as a whole points to some beneficial effects of computer-enabled discharge communication interventions, particularly for the secondary outcomes that we assessed.
Semiquantitative visual assessment of study results
Discussion
To our knowledge, this is the first systematic review to assess the efficacy of computer-enabled discharge communication. With the exception of two studies, the 12 interventions identified generally did not overlap with those described by two reviews done in 2007.2 3 Mortality and readmission to hospital/emergency departments within 6 months appear to be similar for patients regardless of type of discharge summary, although one study found a significant reduction for patients in the intervention group at 12 months. There is limited information about the impact on postdischarge adverse events, as only two studies reported this outcome; one study relied on physician recall of events after 6 months, and the second more rigorously identified events, albeit at only 1 month. More definitive benefits of computer-enabled summaries were identified with respect to improved quality and completeness, timeliness of delivery to care providers, as well as satisfaction among physicians and patients/families.
Our review has several caveats and limitations. Relatively few studies have been carried out in this area, all of moderate methodological quality, with heterogeneous patient populations, measures used and outcomes reported—ultimately limiting our ability to pool results in a meaningful way. Readers will recognise that electronic health records and discharge tools are complex interventions that require interplay between information technologies and human factors in a local context. For example, high rates of medication transcription errors found in traditional discharge summaries can be easily carried over to electronic summaries, and physicians may perceive that greater effort is required to complete these summaries if stand-alone systems are used (that is those not integrated with existing information technology infrastructure and therefore requiring human data entry).9 Also, efficacy in one setting or context does not guarantee a similar benefit in other hospitals or jurisdictions.
A final point to mention is that a number of computer-based interventions were excluded from our review because they were only descriptions of the technology or because only uncontrolled evaluations of the interventions had been reported.23–31 While outside the scope of this review, it would also be pertinent to examine communication of medication information at the time of discharge between inpatient and outpatient pharmacies,32–34 given that information transfer relating to medications is also a particularly vulnerable handoff.33
Should healthcare organisations now move to invest in the establishment of computer-based discharge communication tools based on the evidence that we have reviewed? Or should they dogmatically wait for more definitive research to be published on hard clinical outcomes of interest before investing in such systems? Such questions are challenging ones to answer, because they weigh the realisation that the status quo for discharge communication under usual care conditions is not tenable. Yet, from the standpoint of scientific enquiry, rigorous studies comparing various communication tools versus usual care are still needed to better characterise the efficacy of such tools. A reasonable balance to addressing the tension of scientific enquiry versus the need for immediate health system improvement is for us to state unequivocally that there is (in this review) certainly evidence to support the implementation of such systems now. However, we encourage organisations that move now to implement such systems to also incorporate formal evaluation protocols to expand collective knowledge on their efficacy, and perhaps also their cost-effectiveness. Such an approach would allow health systems to address the clear need for immediate system enhancements, while also potentially contributing new information to the evidence base on such computer-based communication interventions.
Conclusions
In conclusion, our findings globally support the notion that computer-enabled discharge communication tools are beneficial and worth implementing now. However, the evidence in support of their widespread implementation is still relatively limited in scope. Given the rapid uptake and continuing evolution of electronic patient information systems in acute and primary care settings, it is important to continue to scientifically study the extent to which such systems affect patient outcomes.
References
Footnotes
Funding Alberta Innovates – Health Solutions.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.