Article Text

Abstract
Evidence-based medicine (EBM) has been influencing medicine for almost 20 years. It is important because the volume of medical literature available means it is impossible to stay up to date. This article looks at the background and definitions of EBM together with an outline of the tools that can support EBM in practice. Methods of grading the reliability of published articles are discussed. The role of systematic reviews and the utility of forest plots, L'Abbe plots and numbers needed to treat are presented. Some see EBM as a rule book whereas its strengths are in the ability to give tools to assess evidence. While evidence is primarily used for individual patient care, it can also be used for professional interventions and changing systems. Clinical pharmacists are encouraged to develop these skills in their clinical practice.
Statistics from Altmetric.com
Evidence-based medicine (EBM) has been an important and a sometimes controversial topic for almost 20 years, though some would argue that its roots go back to nineteenth century French philosophy. The phrase was almost certainly coined by researchers at McMaster University in Canada in the early 1990s. It is one of those subjects that divided opinions, many because it challenged so-called ‘eminence’-based medicine, especially among senior hospital staff, and has frequently shown that some opinions were just wrong.
EBM is necessary for a number of reasons but the key ones are the following:
There is too much information available to us. Medline, Embase and CINAHL have over 20 million unique papers which translates into a lot of knowledge that most practitioners do not know about. Davidoff, writing in 1995, stated ‘Busy doctors have never had time to read all the journals in their disciplines. There are, for example, about 20 clinical journals in adult internal medicine that report studies of direct importance to clinical practise, and in 1992 these journals included over 6000 articles with abstracts: to keep up the dedicated doctor would need to read about 17 articles a day every day of the year’.1 That situation, if anything, has got worse and applies equally to clinical pharmacists.
Resources are limited and we need to ensure that we are using the most effective and cost-effective medicines. It has often been stated that the most expensive medicine is not some new emerging therapy but simply a treatment that does not work.
In this paper, definitions of EBM will be discussed together with the challenges faced by all involved in the treatment of patients. The tools of EBM will be presented and outlined.
What is EBM?
The time-honoured definition is from Sackett et al2
Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practise of evidence based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research. By individual clinical expertise we mean the proficiency and judgment that individual clinicians acquire through clinical experience and clinical practise.
This is very carefully worded and each of the phrases is important. In clinical practice there is a stated aim of using current best evidence; that means, keeping up to date and applying that evidence using clinical judgement. For example, it is known that oral non-steroidal anti-inflammatory drugs provide good pain relief but clinical judgement dictates that they should usually not be used in patients with gastric ulcers as there is the possibility of inducing a bleed. In addition, there is an integration of individual clinical expertise with best available clinical evidence. This is not ‘cookbook’ or guideline medicine. Clinical skills are vital and clinical pharmacists need to develop these through clinical experience and clinical practice to improve their status and credibility as evidence-based practitioners.
The dimension missing from this definition but added by others soon after is that of patient-reported observations and patient preferences. EBM has to take into account patient preferences and wishes. Medicine works in cooperation with patients and is not something done to them. Take a middle-aged, slightly overweight man who regularly undertakes strenuous exercise. He is advised by his family practitioner to take a statin based on reliable evidence. Within a short period, he notices pain in his legs that is sufficiently bad to discourage him from exercise. In this case he may decide not to take the statin as he may well become more overweight and less healthy by continuing with the statin.
Wisdom and knowledge
Sackett recognises that knowledge alone is not sufficient to practise EBM. The clinical skills required to deliver a clinical pharmacy service develop over time and are learned by interacting with patients. This makes the requirement for pharmacists to become specialists particularly important to stand as consultants on an equal playing field with their medical colleagues.
Sir Muir Gray in his book on Evidence-based Healthcare and Public Health3 divides treatments into three groups: those that do more good than harm; those that do more harm than good; and those of unknown effect. There are many pharmacists who have an inherent faith in the fact that a medicine has a licence and so such a classification will come as a surprise. In fact, Gray goes on to estimate some numbers and suggests that around 50% of treatments do more good than harm and around 10% do more harm than good, which leaves 40% of unknown effect. He argues that probably only about a quarter of that unknown group is being investigated as part of a good quality research programme. Such estimates must have an impact on practice and research. In the first group efforts should be made to promote use, providing they are affordable. In the ‘does more harm than good’ group, efforts should be made to ensure that they are not introduced into practice or if they are currently being used, the use is reduced and stopped. Similarly, for the unknown group, either stop the interventions or initiate research to determine whether they are beneficial or harmful. The tools of EBM outlined below will go some way to sorting these issues out. It is vital that clinical pharmacists understand the potential benefits and harms of the medicines that they either recommend or handle in their practice.
Licensing of medicines is not enough on its own
This work by Muir Gray illustrates that it is wrong to think that just because a medicine has a licence, it will, by definition, work for every patient to their benefit. In the area of my own research in pain, and in particular, neuropathic pain, we are increasingly aware of conditions for which medicines do not work well. We have coined the phrase ‘expect analgesic failure’ to communicate that message to those who treat painful conditions such as fibromyalgia or other neuropathic pains.
Such scenarios make it important for the clinical pharmacist to know their patients and to know their medicines. Patient interaction should be a top priority and should go alongside the interaction with the patient's prescription charts.
The tools of EBM
Grading of evidence
It is important to know the level of evidence that is being used to guide the choice of therapy for an individual patient and for guideline or formulary development. Levels of evidence tables have existed for a good number of years and an example is presented in table 14:
Level of evidence table (Bandolier4)
There is considerable work going on under the acronym GRADE (Grading of Recommendations Assessment, Development and Evaluation)5,6 to further define the criteria for the different types of research and the quality issues that need to be built into such work.
The practical aspect is that practitioners should understand what underpins any recommendations for a medicine to be used. Anecdote is insufficient and may be considered negligent if higher levels of evidence exist and may run contrary to the anecdote! Professor Sackett insisted that his staff looked for systematic review evidence as the primary source and only accepted lesser evidence if that was unavailable. Currently it is estimated that some 2500 systematic reviews are being published every year7 so even restricting our sources to systematic reviews is challenging.
Systematic reviews
If systematic reviews are the most reliable evidence for interventions in healthcare—remember an intervention can be something done by a clinician such as a clinical pharmacy consultation and not just a medicine—then it is important that such research is recognisable and can be appraised.
A systematic review is a research paper based on sound scientific methodology designed to identify, appraise and summarise relevant literature to answer a question. There are a number of key components, which include defining the question in an unambiguous form, clear objectives, defined inclusion and exclusion criteria, a detailed search, an assessment of the quality and validity of identified studies, data extraction from included studies and, if data allow, a meta-analysis and/or other analyses.
The question, objectives and inclusion criteria are typically developed by building a PICO—an acronym for the identification of participants, intervention, comparison and outcomes.
Cochrane has turned the process into something of an industry and the output published on the Cochrane Library8 is generally regarded as being of high standard, though often not easy reading!
Forest plots
A forest plot (see figure 1) is a graphical representation of a meta-analysis which shows a list of included studies with effect estimates and CIs, and is usually presented with a combined estimate of effect—essentially a weighted average. The individual studies are presented as a box and whiskers and the summary result as a diamond. The example is from a Cochrane review of carbamazepine for neuropathic pain.9 Data are presented for three different conditions with an overall estimate of effect.

Forest plot.
In the first subgroup within the figure, three studies are included. The results are combined as a meta-analysis which is represented as a diamond. The extreme points of the diamond represent the CI.
Number needed to treat
Number needed to treat (NNT) is another useful tool that started life in McMaster. They convert a simple statistic—the absolute risk reduction (ARR)—into a clinically useful number by taking the reciprocal of the ARR. NNT is defined as the number of people who have to be treated for one to benefit. Such a tool is useful in several different ways. First, it gives estimates of the effectiveness of a particular intervention, which helps to emphasise the fact that most medicines only work in a proportion of patients. The best NNT is of course when everyone improves with the intervention and none improve with the control. There are treatments that reach this high standard, including anaesthetic agents and antibiotics when used for susceptible bacteria.
The second benefit to practitioners is that NNTs for similar treatments of a given condition can be compared in something like a league table. Recent years have seen the development of the number needed to harm alongside the NNT. This gives an indication of the number of people who may suffer harm (can be defined as minor or major) for a given intervention.
A simple formula is used to calculate the NNT, usually based on randomised placebo-controlled trials, although other comparisons are possible.
L'Abbé plots
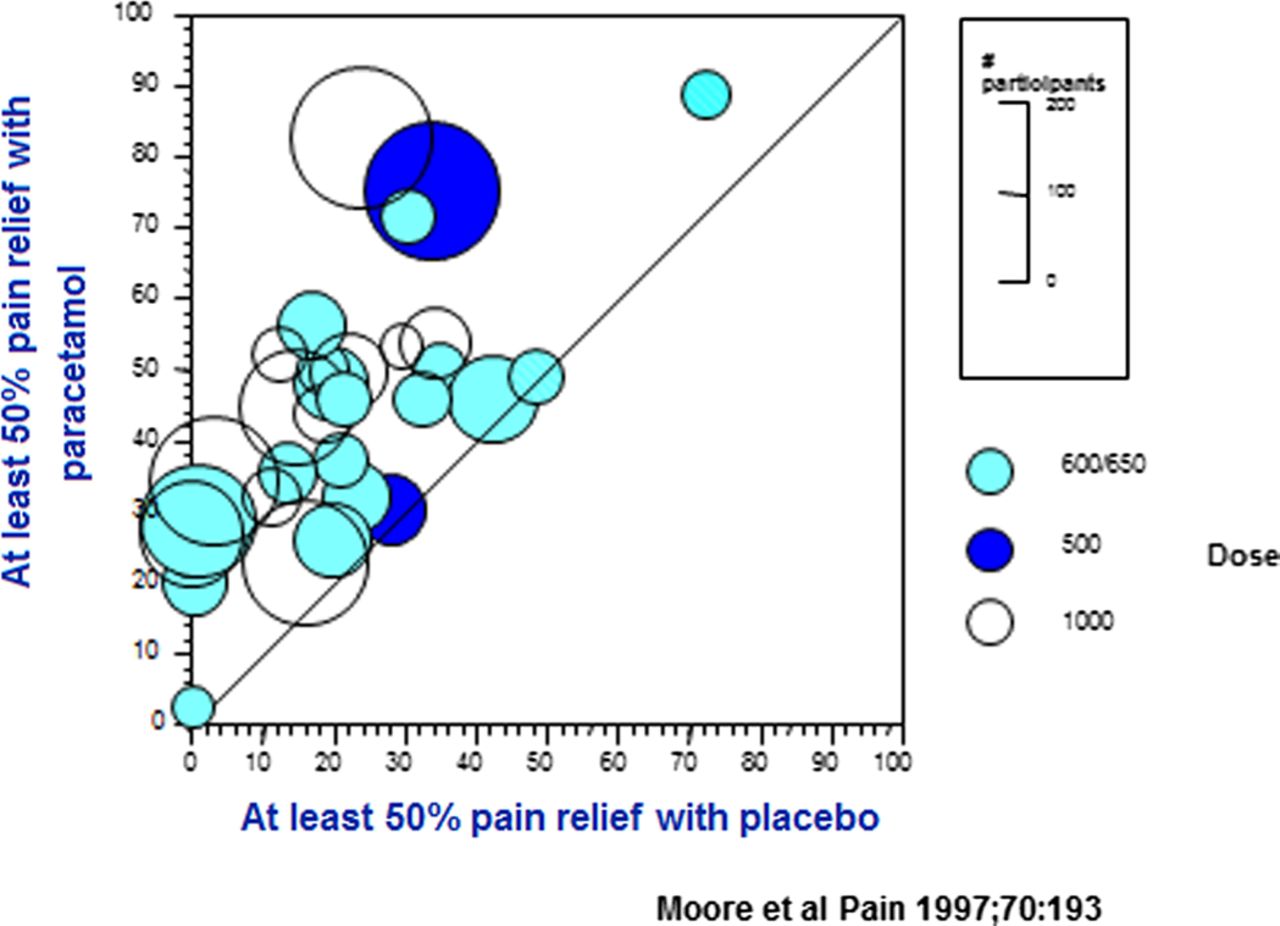
L'Abbé plots are a simple graphical way to present data from multiple studies (randomised controlled trials) if they report dichotomous data to show how they fall on a simple graph.4 The percentage of responders in the treatment arm and the percentage or responders in the control arm are calculated and a point or circle is placed on the diagram to illustrate whether treatment is better or worse than the control. The size of the circle can be made proportional to the size of the study to indicate where the weight of evidence lies (figure 2). An example is shown in figure 3. This plot illustrates that the majority of studies fall well above the line of equality (no difference between active and control). There is no attempt to provide a summary statistic so L'Abbé plots form part of the evidence alongside other summary statistics, such as relative risk or NNT.

Paracetamol in acute pain—single dose.

{kind=link}
{kind=link}
{kind=link}
L'Abbé plot for treatment.Q9
In conclusion, use EBM in your own practice
Above, we noted that Sackett stated that EBM requires the explicit and conscientious use of best evidence. Much clinical pharmacy is practised without such an aim and it is time for change. Pharmacists need to become evidence experts in terms of patient care, developing professional skills and in changing systems. So acquire the skills you do not have and use them. It will positively affect your practice, your patients, your colleagues and your career.
Key message
The huge volume of medical literature makes the use of EBM tools essential if we are to practice effectively.
Pharmacists need to understand and effectively interpret the evidence that underpins their own practice.
Forest plots, NNTs and L'Abbé plots are a means to interpreting evidence reliably.
Acknowledgments
Acknowledgement I am grateful to my colleagues at the Oxford Pain Research Unit who have taught me so much and provided such a fruitful environment in which to work.
Competing interests Phil Wiffen manages his own company called Oxford Systematic Review Services.
Provenance and peer review Commissioned; externally peer reviewed.