Article Text

Abstract
Objectives Cancer patients have a high incidence of concurrent chronic diseases, the pharmacological treatment of which is generally complex and carries an inherent risk of drug-related problems (DRPs). DRPs can interfere with the patient's health outcomes. No systematic investigation of the prevalence of DRPs in hospitalised cancer patients has been performed in Norway. The aim of this study was to characterise the DRPs on an oncology ward, using systematic medication review, and to suggest interventions to optimise drug therapy.
Methods A clinical pharmacist applying the integrated medicines management method reviewed the drug treatment of 48 in-patients. The identified DRPs and the interventions proposed by the clinical pharmacist were discussed with the oncologists and oncology nurses, and the conclusions were characterised.
Results 100 DRPs were identified through medication review. Of these, 41% were identified in the medication charts, 21% by evaluating the choice of drug and 21% by evaluating drug dosing. 75% of the suggested interventions for DRPs were implemented in the drug therapy of the patients.
Conclusions The results of this study demonstrate that the suggested interventions for reducing DRPs were frequently implemented by oncologists. The results also demonstrate that a clinical pharmacist, using medication review on an oncology ward, probably can improve the quality of the drug treatment of hospitalised cancer patients.
- CLINICAL PHARMACY
- PHARMACOTHERAPY
- MEDICAL ERRORS
- CLINICAL PHARMACOLOGY
- INDIVIDUALISED MEDICATION SURVEILLANCE
Statistics from Altmetric.com
- CLINICAL PHARMACY
- PHARMACOTHERAPY
- MEDICAL ERRORS
- CLINICAL PHARMACOLOGY
- INDIVIDUALISED MEDICATION SURVEILLANCE
Background
Errors in drug therapy frequently result in medical interventions having suboptimal effects. In the worst-case scenario, such errors may pose health risks to the patients. Modern cancer treatments often involve combinations of multiple drugs. In addition, there is increasing awareness among oncology professionals that the treatment of co-morbidities can increase the risk of errors in the drug treatment of patients receiving chemotherapy.1 Thus, qualified healthcare professionals should frequently review the drug treatment and the treatment should be tailored to the individual patient. Quality assurance methods such as medication reviews, conducted by clinical pharmacists, have reduced the negative effects of drug-related problems (DRPs) on general medicine wards in Norwegian hospitals.2 A DRP is defined as an event or circumstance involving drug therapy that actually or potentially interferes with the desired health outcomes.3 Moreover, reviews of DRPs indicate how and where improvements can be made in drug therapy. Clinical pharmacy seeks to improve the drug treatment of individuals.4
Integrated medicines management (IMM) is a clinical pharmacy method that is used across Northern Europe.5–7 Studies have shown that a clinical pharmacist involved in a multidisciplinary treatment team applying IMM, may identify a high number of DRPs.8–10 Previous studies have demonstrated that clinical pharmacists can improve supportive treatment for pain and gastrointestinal disturbance among cancer patients.11 ,12 Cytotoxic, biological and immune system-modulating drugs caused 31% of the fatal adverse events reported to the Norwegian Medicines Agency in 2011.13 The introduction of surveillance by clinical pharmacists may help to reduce the impact and frequency of these adverse events. In a study by Yeoh et al,14 a method similar to IMM was used to identify DRPs among hospitalised cancer patients; the patients were more satisfied with their drug treatment after a medication review by the clinical pharmacist. Another study conducted by clinical pharmacists at a university hospital in Sweden, found DRPs in a significant proportion of patients hospitalised for cancer treatment.15 The potential effect of the identification of DRPs on an oncology ward in Norway by a clinical pharmacist has not previously been investigated. Moreover, it is relevant for future studies to determine whether IMM is a suitable method for reviewing medication on Norwegian oncology wards.
The aim of this study was to characterise and estimate the frequency of DRPs identified by a clinical pharmacist conducting medication reviews on a university hospital oncology ward, and to evaluate whether suggested interventions had an impact on the drug treatment of cancer patients.
Methods
Patients on one oncology ward at Radiumhospitalet, Oslo University Hospital, were asked to participate in this study. Patients with a diagnosis of head and neck, lung or skin cancer, or tumours of the central nervous system (CNS) are admitted to this ward. The recruitment period lasted 6 weeks, starting in September 2012. The ability of patients to provide written informed consent for participation was the only criterion for inclusion. The IMM method was applied in conducting a thorough systematic check of pharmacotherapy.5
The current drug use for each patient was reconciled at admission by the treating oncologist combining information obtained from patient interview and from former discharge notes. If the oncologist felt it was necessary, the primary care physician was contacted. The medication review by the pharmacist was performed as a quality assurance check of the medication list on the ward after the oncologist had performed the initial admission. The clinical pharmacist scrutinised the electronic medical record and the drug chart for information relevant to drug treatment. Additional information about patients revealed in discussions during multidisciplinary meetings was also documented and used for identification of DRPs.
Characterisation of DRPs
DRPs were identified and characterised according to the consensus classification described by Ruths et al.3 The presence of an indication for drug therapy, but with no treatment applied, was considered as a DRP, and new treatment options were suggested. All symptoms were evaluated as potential adverse drug reactions, except adverse reactions following chemotherapy; adverse reactions anticipated from cancer chemotherapy were omitted from the DRPs identified in our study. However, if available drugs were not used for supportive care to alleviate adverse reactions, this was registered as a DRP; that is, inappropriate choice of drug. A lack of efficacy and the presence of unexpected adverse reactions were investigated and characterised as DRPs. Supportive pharmacotherapy supplied in conjunction with cancer treatment was evaluated as to whether it was sufficient and in accordance with guidelines, patient characteristics (organ function, age, frailty, laboratory data) and normal therapeutic practice on the ward. The treatment of concomitant co-morbidities was also compared with international or local guidelines. Both patient non-compliance and lack of therapeutic drug monitoring, when identified, was characterised as a DRP. Each drug was assessed for correct indication, dosage and possible interactions with other drugs. Interaction analysis was performed using both the Lexi-Interact and Druid databases.16 ,17 Many of the patients in the ward had impaired swallowing function, mainly because of adverse reactions to cancer radiotherapy, and their medication had to be manipulated before administration. Even though this was a common bedside event, it was seldom documented in medication journals on the ward.
Data collection
For each patient, a medication review form was created and regularly updated with new information about medicines, laboratory results and symptoms throughout their hospital stay. The following information was recorded: age, gender, length of hospital stay, number of medications on admission and the cancer diagnosis. The identified DRPs were recorded, characterised and documented according to the consensus classification described by Ruths et al.3 Appropriate suggestions for intervention for each identified DRP were forwarded to the multidisciplinary team for evaluation. Accepted interventions resulted in amended pharmacotherapy, while unaltered treatment or treatment changed in a different way than suggested by the clinical pharmacist, was noted as a rejected intervention.
Ethics approval and statistical analyses
This study was approved by the Data Protection Officer at Oslo University Hospital and characterised as a quality assurance project by the Regional Ethics Committee in Norway. The study was performed as a descriptive study of quality assurance, identifying DRPs and aiming to identify potential means of improvement. Relevant to this definition, frequency counts were used to determine the quantitative presence of DRPs. Observations were analysed using simple descriptive statistical tools. As such, this is a study for hypothesis generation rather than testing.
Results
Of 115 patients admitted to the oncology ward, 51 were invited to participate in the study. The remaining patients (n=64) were not invited due to the capacity limitations of the clinical pharmacist collecting data. As one patient refused, and two patients could not give written consent because of their health condition, the study included 48 patients. The study population was 50% male. The mean age was 62 years for males and 70 years for females, and 40% of the patients were over 70 years of age. One quarter of the patients were admitted directly from another hospital. The average duration of hospital stay was 10.9 days. Patients with head and neck cancer accounted for 37% of the participants, while patients with skin cancer, lung cancer and tumours of the CNS accounted for 33%, 27% and 4%, respectively. Male participants were predominantly treated for head and neck cancer, while female patients were more often treated for lung cancer. Polypharmacy, defined as the concurrent use of more than five drugs, was identified in 85% of the patients. Some 15% of the patients used 15 or more medications at admission, while the average number of medications was 7.6.
Thirty-five patients (73%) had one or more DRPs identified through the medication review. A total of 100 DRPs were identified, giving an average of 2.1 DRPs per patient or an average of 2.9 in those patients with DRPs. ‘Inadequate drug chart’ was the most frequent type of DRP, contributing 41% of the overall number, while DRP classes ‘Drug choice’ and ‘Dosing’ contributed 21% each. The distribution of the DRPs identified in the study is illustrated in figure 1.
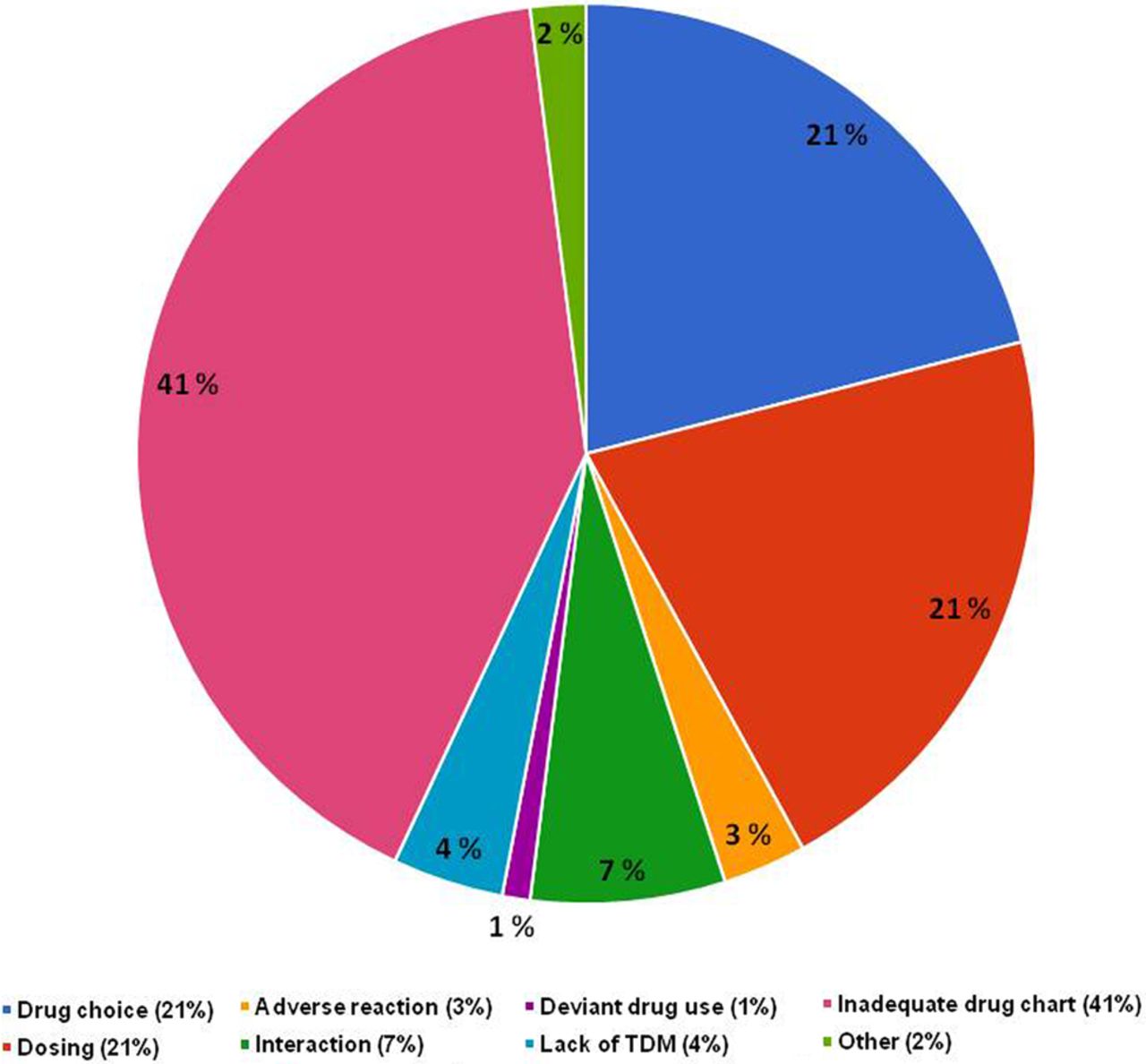
Classification and frequency of drug-related problems. TDM, therapeutic drug monitoring.
Figure 2 shows the distribution of the drugs involved in the DRPs defined according to the main ATC groups.18 Paracetamol (6 DRPs), zopiclone (5 DRPs), oxazepam (3 DRPs) and citalopram (3 DRPs), all drugs acting on the nervous system (ATC group N), were identified in 17 of the 100 DRPs. Pantoprazole was involved in the DRP ‘Need for additional drug’ four times. Dexamethasone was recorded four times as a DRP related to ‘Dosing’ because the hospital guideline had not been updated to reflect current international recommendations. In ATC group C (drugs affecting the cardiovascular system), a wider range of pharmaceutical substances contributed to the 16 DRPs: simvastatin, metoprolol and several angiotensin-converting enzyme inhibitors and loop diuretics.

Number of drug-related problems (DRPs) according to the ATC classification of the drug.
Of the 100 measures suggested by the clinical pharmacist to resolve the DRPs, 75 (75%) were implemented. Only seven of 41 measures proposed to improve medication chart documentation were rejected, while only 4 of 10 measures for DRPs related to presumably low dosing were implemented. Among DRPs associated with changes in dosage, dosing time, formulation and route of administration, 11 of 21 measures were implemented, while the proposed introduction of a new drug was implemented in 10 out of 11 cases. Five measures against potential drug interactions were implemented in treatment, while two were rejected. Figure 3 shows the distribution of measures for the DRPs in relation to whether they were implemented or not.

{kind=link}
{kind=link}
{kind=link}
Classification of drug-related problems (DRPs) identified in the study (n=100, in 35 patients). TDM, therapeutic drug monitoring.
Discussion
In the present study, the clinical pharmacist identified 100 DRPs among 35 (73%) of the included patients, giving an overall frequency of 2.1 DRPs per patient. Among the 100 interventions suggested, 75 were implemented in the ongoing pharmacotherapy of the patients. DRPs related to choice of pharmacotherapy and dosage occurred frequently in hospitalised cancer patients.
Interventions suggesting different treatment options were implemented quite often (18 of 21 interventions), while the oncologists more often rejected interventions suggesting different dosages (10 of 19 interventions). It is plausible that the addition of new treatment was perceived as more proactive than adjusting the existing dosage of established therapy.
Comparing our results with former studies provides insight as to whether medication review is an effective method to ensure quality in drug treatment on oncology wards. The present study was conducted on an oncology ward where a clinical pharmacist had not been systematically involvement previously. Two medication review studies conducted among cancer patients are relevant for comparison, one by Bremberg et al from Sweden and another by Yeoh et al fro-m Singapore.14 ,15 The study from Singapore had a longer observation time and larger sample size, while the Swedish study was comparable in size and length of observation period with our study. While ‘drug interactions’ and ‘adverse reaction’ were the most frequent DRPs identified by Yeoh et al, these DRPs were not observed as often in our study. Differences in the applications for interaction checks may contribute to the differences in these observations. The Swedish study presented observations comparable to our study regarding the number and frequency of DRPs per patient. Compared to our results, the studies of Bremberg et al and Yeoh et al both had fewer interventions proposed and implemented. Differences in the cancer diagnosis of the included patients may have contributed to these discrepancies.
Compared to the number of DRPs previously reported from hospital wards in Norway, we identified a somewhat lower frequency of DRPs. The study by Buajordet, conducted on a ward for patients with rheumatic disease, identified four DRPs per patient and 87% of the patients had DRPs identified in their drug treatment7 compared to 2.1 DRPs per patient and 73% of patients in our study. The frequency of the DRPs concerning ‘choice of drug’ was 21% in both studies. In a study by Blix et al describing DRPs from internal medicine wards, 2.1 DRPs were regarded as clinically relevant per patient.19 For comparison, 1.6 DRP interventions per patient were implemented in our study.
The fact that the number of identified DRPs in our study among cancer patients is lower than the expected number of DRPs in patients acutely admitted to internal medicine wards might be explained by a high proportion of the cancer patients being hospitalised for elective cancer radiotherapy and being generally preparedness for hospitalisation. It is important to mention that the frequency of ‘non-optimal formulation’ DRPs is probably underestimated in our study. Deviant drug administration by patients and healthcare professionals might have been detected to a lesser degree. The proportion of drugs that were manipulated (split, crushed or dissolved) was particularly large in patients with head and neck cancer. These drugs were often listed in the medication chart with several optional formulation forms, and the study was not designed to observe actual bedside administration of the drugs.
Despite the limitations noted above, this study indicates that IMM, with further optimisation, could be a suitable model for clinical pharmacy practice and an adequate method for similar studies on oncology wards.
Conclusion
The clinical pharmacist identified 100 DRPs in the drug treatment of 48 patients. One or more DRPs were identified in 35 (73%) of the patients during the study. In this population of hospitalised cancer patients, the most frequent DRPs were related to the selection of drugs and drug dosage. Drug treatment was changed as a result of interventions suggested by the clinical pharmacist in 75% of cases. Recognition of risk factors, the frequency and the characteristics of DRPs was important in the improvement of drug treatment of individual patients. A suggestion to increase or decrease the dosage was the intervention most frequently rejected by clinicians (10/19), while interventions suggesting different treatment options were often implemented (18/21). The results from this study demonstrate how the involvement of a clinical pharmacist with expertise in drug treatment on an oncology ward conducting medication reviews, could increase the quality of drug treatment.
Key messages
What is already known on this subject
Quality assurance methods, such as medication reviews, implemented on general medicine wards in Norwegian hospitals have reduced the number of drug-related problems (DRPs).
The occurrence of DRPs has not been systematically investigated among hospitalised cancer patients in Norway.
The potential effect of the identification of DRPs on oncology wards in Norway by a clinical pharmacist has not been investigated.
What this study adds
Substantial numbers of DRPs were identified among hospitalised cancer patients in this study.
The results demonstrate that the interventions proposed by the clinical pharmacist in order to reduce the number of DRPs were frequently implemented by oncologists.
Acknowledgments
The support of the staff on oncology ward A7 at Radiumhospitalet is greatly appreciated, as is the patience and willingness of patients to participate in this study.
References
Footnotes
Competing interests None.
Ethics approval The Regional Ethics Committee (REK) HELSE SØR ØST HF Norway approved this study.
Provenance and peer review Commissioned; externally peer reviewed.