Article Text

Abstract
Objectives Over the last decades, several papers have evaluated clinical pharmacy interventions in hospital settings with conflicting findings as results. Medication reviews are frequently a central component of these interventions. However, the term ‘medication review’ covers a plethora of principles and methodologies, and the practical procedure is seldom described in detail, which makes reproducing study findings difficult. The objective of this paper is to provide a detailed description of a procedure developed and used for pharmacist-led medication review in acute admissions units.
Methods A procedure was developed based on clinical experience and inspiration from previous studies and literature on medication review models. The procedure was developed to fit the busy workflow in acute admissions units.
Results The procedure consists of five steps: (1) collection of clinical patient data, (2) collection of information about the patient's medical treatment, (3) patient interview, (4) critical examination of the patient's medications and (5) recommendations for the hospital physician.
Conclusions We have provided a detailed description of a procedure for pharmacist-led medication review. We do so, not to provide or advocate a single one-size-fits-all solution, but in an attempt to inspire a debate of the practical approach on how to execute a systematic medication review in order to develop and expand clinical pharmacy and achieve better patient outcomes.
- CLINICAL PHARMACY
- Hospitals
- Acute admissons units
- clinical pharmacists
- medication review
- patient-centered
- systematic procedure
Statistics from Altmetric.com
- CLINICAL PHARMACY
- Hospitals
- Acute admissons units
- clinical pharmacists
- medication review
- patient-centered
- systematic procedure
Introduction
Over the last decades, several papers have evaluated an array of pharmacist-led interventions in hospital settings, and they have shown improvement in pharmacotherapy, reduction in medication-related readmissions and reduction in healthcare costs.1–3 No effects on mortality and all-cause readmissions have been identified.1–3 Medication reviews are frequently a central component of such interventions, often delivered in combination with other services.2 However, the term ‘medication review’ covers a plethora of principles and methodologies4–7 and often uses a range of tools to assess inappropriate prescribing.8–11 Such tools are often aimed at specific diseases and provide explicit guidance regarding single interventions. However, many important medication-related problems fall outside their scope, and as such explicit tools can provide an aid for expert medication review, but cannot stand alone or replace clinical judgement.11
When assessing the pharmaceutical literature, the actual procedure for conducting medication reviews is seldom described in sufficient detail to enable readers to reproduce the method or, more importantly, implement the intervention in other settings. As an example, a recent systematic review could in 18 out of 31 studies not even determine if the pharmacists’ recommendations were passed on to the physician orally or in writing.2 A few, more recent, studies have published their methodologies in detail, one specific to the hospital setting,12 one specific to a primary care setting13 and one which can be used in both settings.14 The setting will likely influence the procedure for medication review, due to variations in access to the full medical record, laboratory results and contact with the physician and patient. Furthermore, acutely admitted patients are often severely ill, which is a known risk factor for medication-related problems.15
In order to develop and expand clinical pharmacy, there is a need for a thorough debate about practical and specific procedures when conducting medication review in the hospital setting. This paper presents an example of a medication review service provided at acute admissions units, in an attempt to initiate a debate on the practical procedures for pharmacist-led medication review.
The objective of this paper is to provide a detailed description of a procedure developed and used for pharmacist-led medication review in acute admissions units.
Methods
Development of the procedure
We used the definition on ‘medication review’ from Pharmaceutical Care Network Europe as “an evaluation of patients’ medicines with the aim of managing the risk and optimizing the outcome of medicine therapy by detecting, solving and preventing medication-related problems, which could possible lead to harm for the patient”.7 Bearing this definition in mind, two pharmacists (TG and DKB) working as clinical pharmacist for 2 and 7 years, respectively, developed the procedure based on their clinical experience as well as input from other clinical pharmacists with experience in conducting medication review. Two recent systematic reviews1 ,2 were assessed to identify procedures used in other studies (table 1). Of the 13 controlled studies included in these reviews, five studies provided detailed descriptions on their intervention, which were used as inspiration for our procedure.16–20 Two of these studies did not give the impression of using a standardised procedure16 ,20 and only one study had a figure with details of the procedure.17 TG and DKB discussed these various procedures until they reached consensus about how medication reviews could be conducted in an acute admissions unit. It is known that many prescribing errors are found on patients’ admissions,21 therefore we find admission to be a relevant time to perform a medication review. The acute admissions units receive patients from various medical specialties and patients’ spend a maximum of 48 h before being transferred to a hospital department or discharged.22 The procedure was developed to fit into hospital units where physicians obtain the medication history and conduct medication reconciliation when patients are admitted. The hospitals had electronic medical records. The pharmacists performed the medication review shortly after a patient had been admitted and the medication review should therefore not be too time consuming, as the procedure had to fit into the busy workflow of an acute admissions unit.
Data from two recent literature reviews on the procedure for medication review in the hospital setting
Reasons for choosing this particular procedure
Patient characteristics
To perform the most comprehensive type of medication review, the entire medical record, including laboratory results, was examined to assess the characteristics of the patient. Updated laboratory results should be available before performing the medication review, since these are among the five most important factors when considering the medical treatment.23
The patients’ medical treatment
When assessing the patient's current medications, several sources of information should be used to have as many details as possible, since it is known that medication lists are often not complete or correct.24 The medication review requires access to the patient's electronic medical record and the shared medication record, which is an updated medication list including all prescriptions filled at Danish pharmacies within the last 2 years (http://www.fmk-online.dk). Other sources of information, such as the general practitioner, nursing home or the community pharmacy, might also be asked for information about the patient's medications.
Patient interview
A patient interview adds information about the patients’ adherence and attitudes towards medication and possible adverse effects and therefore it was chosen that a patient interview should be part of this procedure whenever possible.
The preliminary list of medications should be used as a starting point for the interview. The focus of the interview was to discover which medications the patient actually takes, including how and when, together with problems related to the medical treatment. Despite physicians performing medication reconciliation upon admission, the medical treatment was consulted with the patient to make sure the medication review was performed on the medications the patient actually takes.
Critical examination of the medical treatment
To ensure a systematic approach, both the entire medical treatment and each individual drug should be assessed. First, the patient's diagnoses were compared with the medications to ensure that all diagnoses and symptoms were treated properly and that the patient was not receiving unnecessary medications. Second, all medications are examined individually to ensure that every single medication is properly prescribed and taken.
In the procedure, not only established adverse drug reactions were sought solved, but also medication-related problems that had not yet caused harm to the patient were communicated to the physician.
Communication with the hospital physician
Action on the recommendations from the medication reviews should be taken by the hospital physician. Whenever the pharmacist could solve the medication-related problem directly through counselling of the patient, this should be done, for example, by helping the patient with practical questions about medication or advice on time of administration.
The primary way of communicating recommendations to the hospital physicians was via the medical record. This is the way hospital physicians communicate and receive information on the patient from other colleagues as well. As the acute admission units have a high patient turnover, the medical record was considered the most appropriate way and would not interrupt the physician while he/she was tending other patients. If the medication-related problem was acute, the pharmacist should in addition take contact to a physician whenever possible.
When conducting medication reviews, minor medication-related problems can be found in almost every hospitalised patient. However, it was chosen that issues concerning cost savings and other issues that were found unlikely to harm the patient would not be commented on in the acute setting. This was found important since it was expected to give a better cooperation with the physicians and prevent ‘alert-fatigue’. Recommendations were defined as clinically relevant, when the pharmacist found that the patient could potentially be harmed if the medication-related problem was not resolved.
Test of the procedure
The procedure described has been pilot tested in two acute admissions units and afterwards implemented in two randomised controlled trials (RCTs) of pharmacist-led medication review at acute admissions units in Denmark. The two units comprised a 16-bed ward at Aarhus University Hospital and a 37-bed ward at Hospital South West Jutland. These units receive patients from different medical specialties. The patients’ spend a maximum of 48 h in the emergency department before being transferred to a hospital ward or discharged.22 The results from the two RCTs will be presented in later publications.
Results
The procedure for systematic medication review consists of five steps (figure 1):
Collecting clinical data
Collecting information about the medical treatment
Performing patient interview
Performing critical examination of the patient's medications
Reporting recommendations to the hospital physician
Collecting clinical data
From the patient's medical record, information concerning the actual hospitalisation is collected:
Basic characteristics (age, gender, residence, smoking status, alcohol use, mental state).
The reason for hospitalisation.
Comorbidities.
If the patient has any previous admissions.
Symptoms that might be attributed to the medical treatment (ie, adverse drug reactions).
Medication allergies.
The results from physical examinations (blood pressure, weight).
Laboratory test results (eg, electrolytes, kidney and liver function, haemoglobin, cholesterol).
The physician's plan for the present hospitalisation.
Collecting information about the medical treatment
From the patient's medical record, the shared patient record and the general practitioner, nursing home or community pharmacy if relevant, the following is obtained:
Medications prescribed to be taken at home.
Changes in the medical treatment at the hospital.
Based on this, a preliminary list of the patients’ medications is created.
Performing patient interview
Among patients who are able to cooperate, an interview is performed. If the patient brings along his/her own medications, these are examined. To facilitate the interview, a checklist of items that should be addressed is followed:
Use of medications, including prescription medication, over-the-counter medicines and complementary medicines.
Medication adherence.
Practical medication use, including difficulties with handling medications.
Any recent changes in the medical treatment.
Indications for the medical treatment.
Symptoms that might be related to adverse drug reactions, with a specific focus on common symptoms like pain, constipation and dizziness.
Previous medication allergies.
Performing critical examination of the patient's medications
Before starting the medication review, a complete medication list is obtained from the preliminary list and the patient interview. The complete list and the patient's comments are now examined, first comparing medical treatment versus the patient's clinical status, diagnoses and symptoms. Afterwards, each medication is assessed individually.

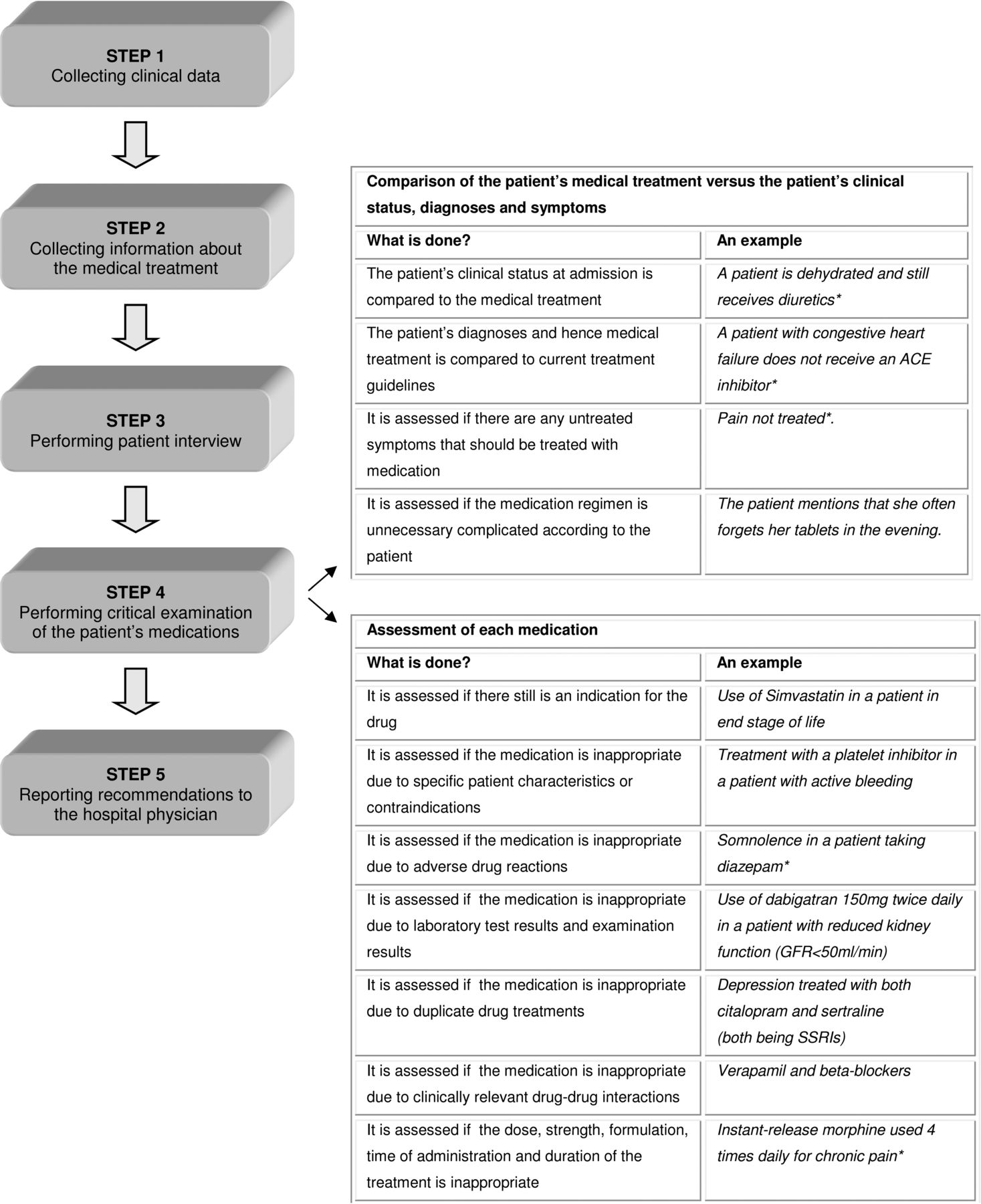{kind=link}
Simplified procedure for systematic medication review in five steps with description of how the patient's medications are examined. *It is examined if there is a reason. Information from previous admissions and ambulatory controls is taken into account. GFR, glomerular filtration rate; SSRIs, selective serotonin reuptake inhibitors.
Pharmacological and pharmaceutical literature is used, such as the Summary of Product Characteristics (http://www.ema.europa.eu), databases of drug interactions (ie, http://www.interaktionsdatabasen.dk), studies on specific medications (from http://www.pubmed.gov) together with national and international treatment guidelines from medical societies and from the Danish Institute for Rational Pharmacotherapy (http://www.irf.dk) which provides healthcare professionals with independent information about medical treatment.
In figure 1, a full description of this step is shown, including examples.
Reporting recommendations to the hospital physician
In this procedure, all recommendations decided to be clinically relevant are documented via the electronic medical record. If the problem is deemed acute, the note is accompanied by oral communication with the physician. The written record contains a description of the problem for the patient and a proposal for solving the problem.
Discussion
We have provided a detailed description of a procedure for pharmacist-led medication review. We do so, not to provide or advocate a single one-size-fits-all solution, but in an attempt to inspire a debate of the practical approach on how to execute a systematic medication review in different settings. In our experience, this procedure is usable in the setting of acute admissions units, allowing us to identify clinically relevant medication-related problems, and still fit in the acute hospital setting with a busy workflow.
A strength of this procedure is that the pharmacist sees the patient after the physician has provided the diagnoses and at a time where results from laboratory tests are available. This enables the pharmacist to perform a more comprehensive medication review, as the pharmacist has more information available. In other models proposed for medication review in the acute hospital setting, the pharmacist meets the patient before the physician,12 which adds the element of obtaining the medication history and to conduct medication reconciliation before the actual review can be performed. A recent Danish study has shown that more medication-related problems are found, when medication reconciliation is also performed, but that the clinical importance is largest for problems found during medication review.24 Another Danish study has reported increased acceptance rates among medication-related problems of high clinical significance.25 As such, we focused on the clinically relevant medication-related problems, which are equivalent to the problems with highest, high and medium priority according to Sexton et al6 As an example, we would not change an already initiated otherwise efficient treatment not showing adverse effects, even though it does not follow current guidelines. Similarly, we will not change regimens for economic reason if it does not affect the patient.
The presented procedure is based on the methods developed and used by two clinical pharmacists. This can be considered a limitation to the paper. However, it is important to emphasise that the model is intended to inspire a debate, not to represent the only correct way of conducting pharmaceutical medication reviews. One limitation to this procedure is that the systematic approach might be time consuming compared with checklists like Beer's Criteria8 or Screening Tool to Alert doctors to Right Treatment (START)/Screening Tool of Older Person's Prescriptions (STOPP).26
The focus of medication reviews is dependent on the setting in which they are performed. In the acute admissions unit, there is a focus on the complaints presented on admission and whether this might be related to the medical treatment. Medication reviews performed later in the patient's hospital stay could have other foci. A model comparable with ours has been described in a general practice setting27 and is currently used in a Danish large-scale project of medication reviews in nursing homes. Compared with the medication review in general practice, the hospital physicians are more interested in the medication-related problems relevant to the actual hospitalisation, whereas they are more reluctant to change the patients’ long-term treatment initiated by the general practitioner.28 On the other hand, the general practitioner would not change a treatment where the responsibility was believed to lay at the hospital physician.27
In this paper, we have presented in detail our procedure for systematic medication review. Hereby we hope other healthcare professionals will provide descriptions on how they conduct medication reviews in order to develop and expand clinical pharmacy and achieve better patient outcomes.
Key messages
What is already known on this subject
Medication review covers a plethora of principles and methodologies.
The practical procedure for pharmacist-led medication reviews is rarely described in sufficient detail to allow methodological assessment or replication.
What this study adds
This paper presents a systematic procedure for medication review described in detail.
By sharing our practical approaches we hope to further develop and expand clinical pharmacy leading to better patient outcomes.
References
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.