Article Text

Abstract
Objectives The European Statements baseline survey was designed to give an insight to how well the European Statements of Hospital Pharmacy (the Statements) are being implemented and to help inform the European Association of Hospital Pharmacists (EAHP) implementation strategy for the Statements.
Methods The online questionnaire was sent to all hospital pharmacies in EAHP member countries. More than 1000 pharmacists completed the survey, which was analysed by Keele University and presented to EAHP.
Results The survey provided general data for each country about the staffing levels and skill mix within each hospital, how well each hospital was implementing each Statement and finally about what were the barriers to implementation for European hospital pharmacists. The survey identified that, generally, the sections covering more traditional roles of hospital pharmacists (procurement, compounding) were being well implemented—96% of respondents indicated that their hospitals had clear processes in place around the procurement of medicines; 91% indicated “When medicines require manufacture or compounding, we either produce them in our hospital pharmacy or we outsource to an approved provider”. Compared with that, clinical pharmacy services, multidisciplinary approaches and active engagement in education and practice research activities are challenging areas in most EAHP member countries. In only 29% of hospitals, the pharmacists enter all medicines used onto the patient's medical record on admission. 49% of responders agreed that the pharmacists in their hospital routinely publish hospital pharmacy practice research. Insufficient capacity and capability in terms of staffing and resources seemed to be main reasons given for low implementation of some of the Statements.
Conclusions After analysis of data from more than 1000 questionnaires, EAHP gained a necessary overview of Statements implementation level and barriers to implementation, needed for informed and efficient progress of EAHP implementation projects.
- EAHP
- Hospital Pharmacy Practice
- European Statements of Hospital Pharmacy
- Survey
Statistics from Altmetric.com
Introduction
European Association of Hospital Pharmacists (EAHP) has conducted surveys of hospital pharmacy practice in European countries since 1995. EAHP surveys have always been a useful source of information about status of the profession within the EAHP membership. The surveys were issued in a 5-year cycle until 2010.
Much has changed in these years, from technical possibilities of conducting surveys to the EAHP itself, in terms of membership and EAHP's activities and projects. In 2014, the European Statements of Hospital Pharmacy were prepared and approved, expressing commonly agreed objectives which every European health system should aim for in the delivery of hospital pharmacy services.1 Once the Statements were published, the second phase of the journey in EAHP's aim to support the best achievable level of practice was to assess how well these were being implemented and what were the barriers and drivers for this. Active support of the implementation of the Statements is one of the most challenging and most important of EAHP's current projects. The journey has a clear target, but one cannot easily aim at a target without knowing the current position and tracking the progress. Therefore, the EAHP agreed that the EAHP survey be repurposed to inform implementation, instead of as overall source of information about hospital pharmacy in Europe.2
Methods
Based on the new purpose of the survey and feedback received from the membership (mainly via delegates participating in the workshops held during EAHP General Assemblies in the past few years), the EAHP Board of Directors agreed to form a new survey working group and commissioned the School of Pharmacy at Keele University team to support this process and conduct the surveys. The survey group then drafted a new concept of EAHP surveys based on the EAHP Statements, using its wording and glossary3 to formulate questions with the proprietary tool Survey Monkey used to conduct the online surveys. The agreed method was to have two levels of survey—(1) a ‘baseline survey’ to find out the current status quo of our professional practice in Europe and monitor progress across all of the Statements and (2) ‘statements survey’ where an in-depth survey would be conducted to provide greater insight into the EAHP members’ efforts to implement the Statements.
The baseline survey covered all six sections of EAHP Statements and will be repeated every 3 years, while the statements surveys are planned to be issued annually in a 2-year cycle, focusing on three of six statements’ sections every year (figure 1).
European Association of Hospital Pharmacists (EAHP) surveys model.
This article focuses on the results of EAHP baseline survey, while the results of the first statements survey will be published later this year. More about the methods of baseline survey can be found in the article by Underhill and Gibbons.4
Results
Section A: results of the general questions regarding hospital activity
This section has focused on the identification of hospital types, staffing, the number of beds served by hospital pharmacy and so on.
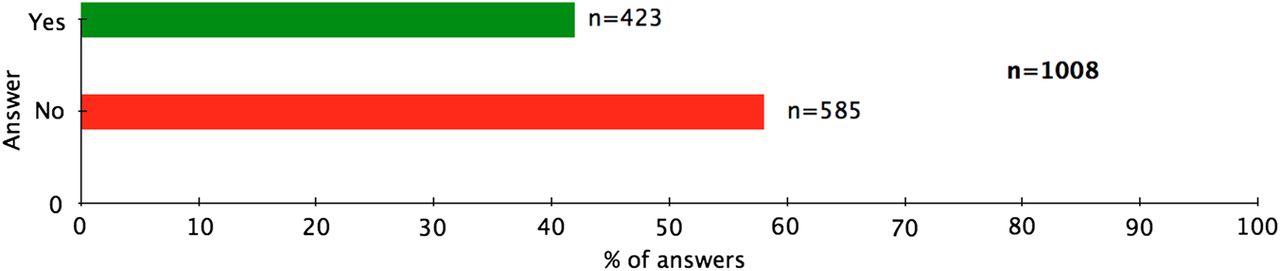
From the responses received, 423 hospitals (42%, n=1008) were declared as teaching hospitals, while 585 (58%) as non-teaching hospitals. The numbers from some countries show that more colleagues from teaching hospitals than non-teaching hospitals answered the survey (eg, Germany 87% and Spain 62%) (figure 2).

Percentage of teaching hospitals in the sample.
Likewise, 71% of hospitals were declared as general hospitals. The survey used the following definition to describe general hospital: “General hospital is a hospital not specializing in the treatment of particular illnesses or of patients of a particular sex or age group, having at least following departments/specializations: Internal medicine, surgery, gynaecology”. The most common responses relating to ‘Other’ were cardiology hospitals, rehabilitation hospitals or multidisciplinary hospitals (figure 3).

Percentage of general hospitals in the sample.
Looking at the number of beds served by hospital pharmacies, half of them reported they served 101–500 (n=503; 50%) and a quarter of them 501–1000 beds (n=247; 25%) (figure 4).

The number of beds served by hospital pharmacies.
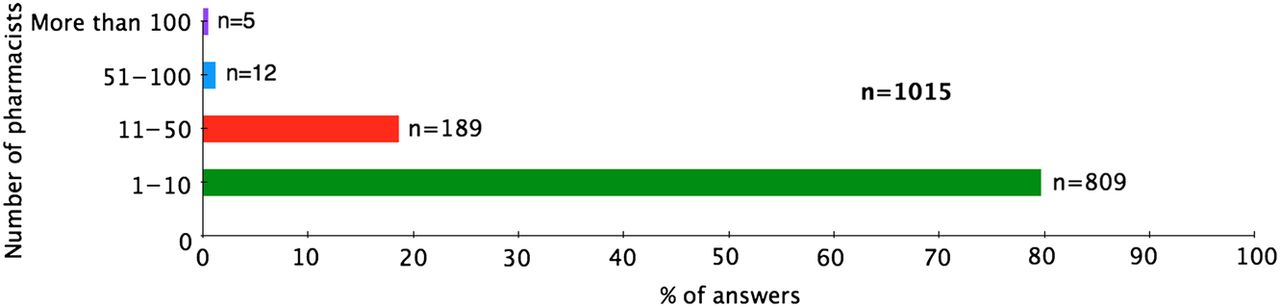
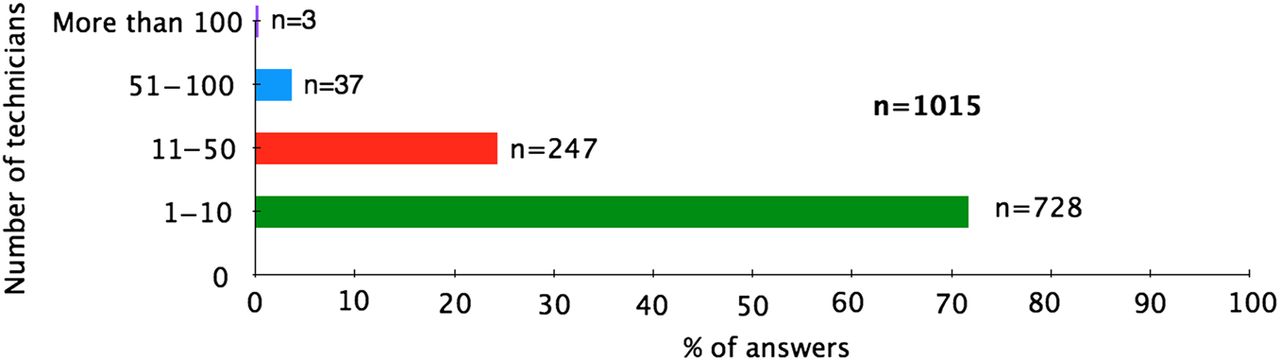
The staffing levels were also examined. Four of five hospital pharmacies in the survey (n=809; 80%) only have 10 pharmacists or less (figure 5). Very similar are the numbers of pharmacy technicians in the pharmacies: 72% of them having less than 10 pharmaceutical technicians (figure 6).

Staffing per hospital pharmacy: pharmacists.

Staffing per hospital pharmacy: technicians.
The majority of respondents (58%, n=612) reported that the chief pharmacists in their hospital are responsible to the hospital chief executive manager/director.
Section B: results of the EAHP Statement questions
In order to fulfil the intended purpose of the survey and find out the status of the profession in relation to European Statements and to identify the Statements possessing the largest implementation challenge, the investigators compared the results of all Statement-related questions. The authors divided the answers scale on the respective questions into two categories—positive or neutral (3–5 on used scale) and negative (1–2 on used scale). The questions were compared by percentage of negative questions. (Please refer to the later paper4 in this issue for more information about questions and used Likert scale. Please also note the question numbering key—first two numbers refer to the Statement number, eg, S21 refers to the Statement S2.1). The graph shown in figure 7 shows the percentage of negative answers by respective questions. Therefore, a higher bar means the question had more negative responses, that is, Statements where responders are saying they are having difficulty complying.
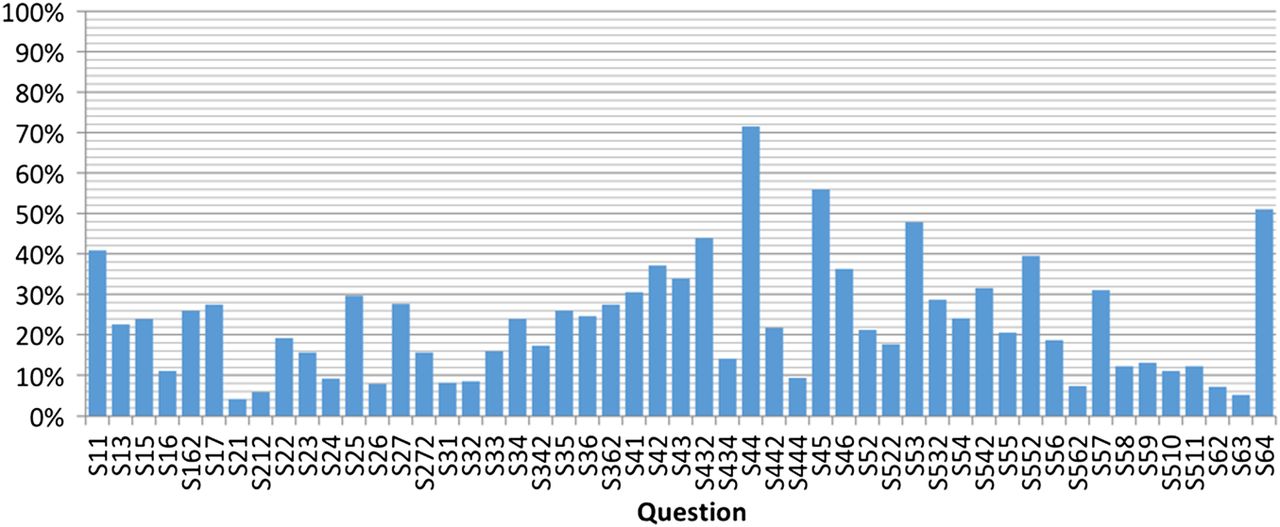
Percentage of respondents who indicated they had difficulty complying with Statement (negative responses).
As apparent from the graph, there is a great variance between responses (and therefore Statement implementation level), raising from 4% (S21: Our hospital has clear processes in place around the procurement of medicine, 96% implementation.) to 71% (S44: The pharmacists in our hospital enter all medicines used onto the patient's medical record on admission, 29% implementation.) There are first level questions with the highest and lowest number of negative responses for each section of Statements summarised in tables 1 and 2 (first level—the first question asked per every Statement, which had to be answered by all survey responders).
The most and least implemented Statements in every section of EAHP Statements
Questions with lowest number of negative responses—the most implemented
B1: focus on those Statements where there were fewer barriers to implementation
Although the primary focus of the survey was to identify those European Statements of Hospital Pharmacy where compliance was difficult and to identify the barriers to their implementation, the same method was used to identify which Statements are currently being implemented widely across Europe.
For each country, all of the questions in the survey were ranked in order of how many ‘negative responses’ they received. The questions in the table below were not placed in the bottom five for any country. Additionally, the table shows the overall proportion of negative responses the questions received. This leads to the conclusion that questions listed in this table, and the European Statements of Hospital Pharmacy that they relate to, are already being implemented to a significant level across every country surveyed.
B2: focus on those Statements where the barriers to implementation were greatest
During the results evaluation, the authors identified five questions that received the most negative responses and were thereby deemed to represent those Statements where the implementation seemed to be most challenging. The authors focused more on these questions, trying to identify the differences in implementation level between EAHP member countries. Table 3 displays the questions with lowest level of implementation, showing not only the mean percentage of negative responses, but also the number of countries that placed the respective questions in their bottom five questions in terms of implementation level.
Questions/Statements with lowest implementation level
Question S44 was related to the Statement 4.4: All the medicines used by patients should be entered on the patient's medical record and reconciled by the hospital pharmacist on admission. Hospital pharmacists should assess the appropriateness of all patients’ medicines, including herbal and dietary supplements. As apparent in figure 8, the variance between EAHP member countries was generally very high, from (almost) full implementation (the lowest bars on the graph) to zero implementation, with 11 countries with 90% or more negative responses (figure 8).
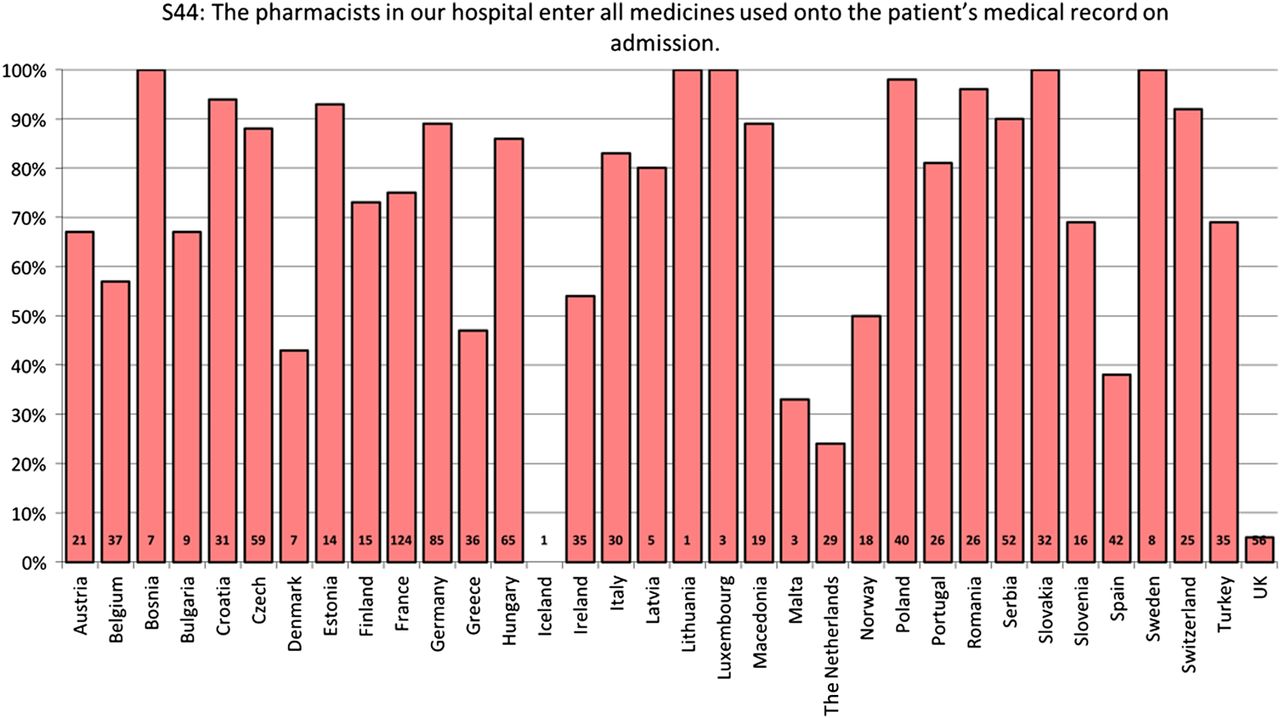
S44: Percentage of negative responses per country.
The respondents named as the barriers, for example, lack of access to patients’ health records and no direct contact with patients, but most commonly they explained that this competence is fulfilled by other healthcare professionals in their hospitals. Furthermore, even the countries where rising level of implementation can be expected in the near future, like Norway, explained that not enough staff and limited service time of hospital pharmacies appear to be problems in successful implementation.
UK and Iceland (although only one respondent) seem to have few issues in complying with this Statement.
Question S45, related to EAHP Statement 4.5 (Hospital pharmacists should promote seamless care by contributing to transfer of information about medicines whenever patients move between and within healthcare settings) shows quite similar distribution of implementation, although generally a bit higher. UK, the Netherlands and Iceland seem to play a role of leaders here too (figure 9).

S45: Percentage of negative responses per country.
The implementation barriers named by the responders were again similar to question S44, such as lack of appropriate IT/software tools, insufficient staffing, poor connection between ward and pharmacy teams or duties were fulfilled by other healthcare professionals. Some responders also stated that there was no reason for pharmacists to contribute to the transfer of information, because this was happening automatically, for example, by fully electronic patients’ records. Some countries (France, Serbia) also indicated that projects to support the implementation of medication reconciliation on patient discharge were at the planning stage.
Question S64 was related to EAHP Statement 6.4: Hospital pharmacists should actively engage in and publish research, particularly on hospital pharmacy practice. Research methods should be part of undergraduate and postgraduate training programmes for hospital pharmacists. As apparent in figure 10, the level of compliance with the Statement is generally more flat; the differences between countries are less pronounced.
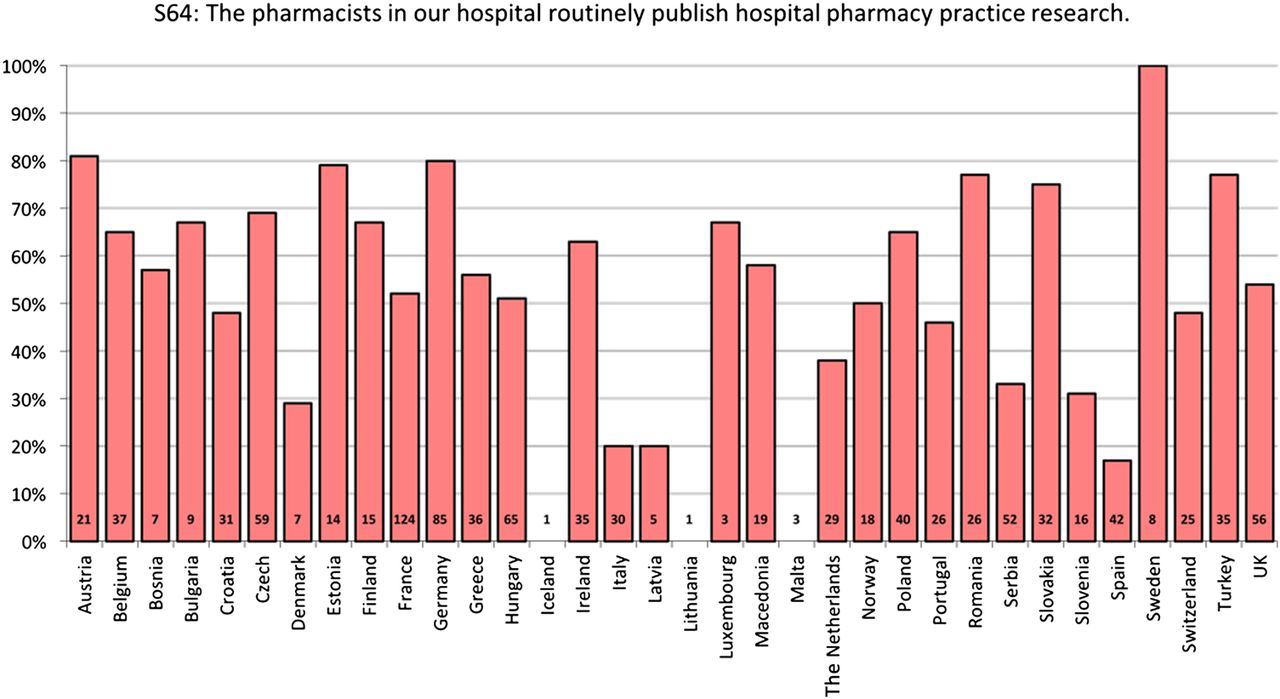
S6.4: Percentage of negative responses per country.
Hospital pharmacists from Spain and Italy seem to be most involved in publication activities, an observation supported by the number of posters presented at EAHP congresses every year, as well as colleagues from Malta and Latvia. Many reasons were given as to why pharmacists seem to be hesitating to publish their practice research. Apart from reasons related to a lack of capacity, one of the general reasons given was the traditional role of pharmacy as a ‘service department’ which is not much involved in the research activities even in the university or teaching hospitals. Pharmacists said they were less motivated to publish research, because there are less incentives and support for them to publish. In some countries, more publications were provided by students as residents, as this probably was often part of their residency programmes.
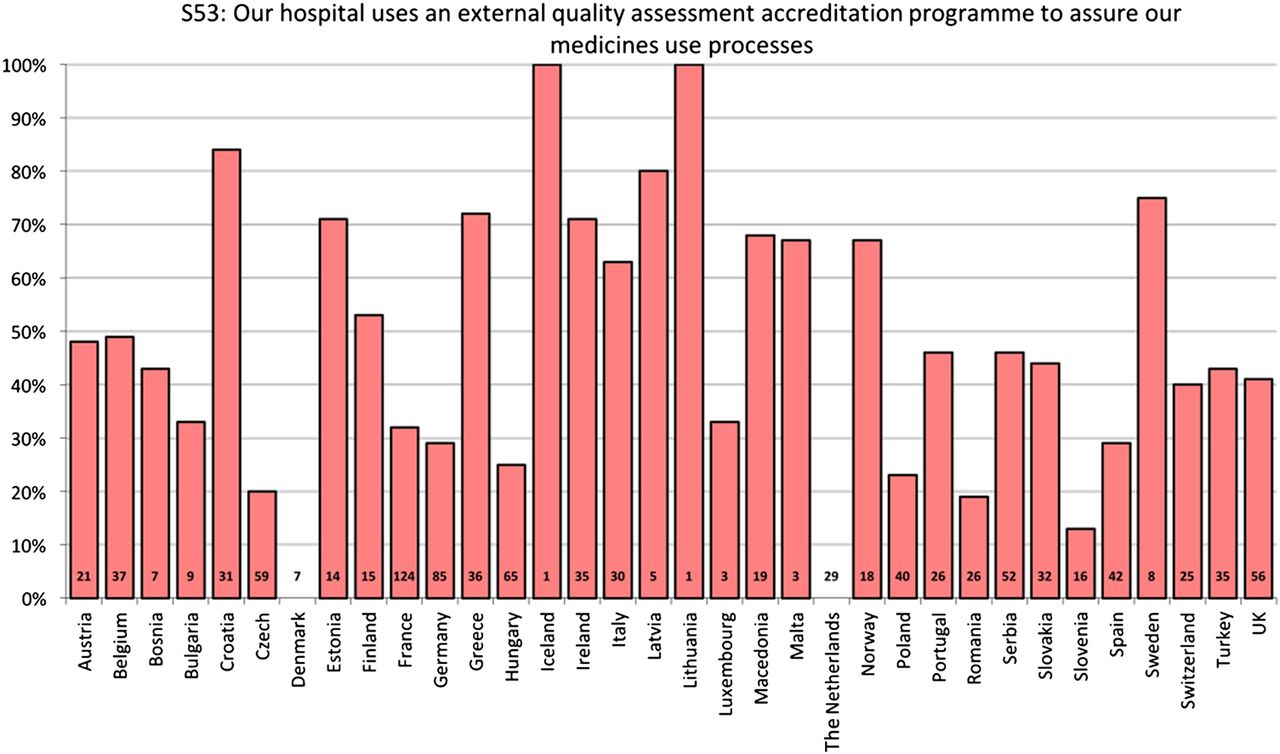
Question S53 was related to EAHP Statement 5.3: Hospital pharmacists should ensure their hospitals seek review of their medicines use processes by an external quality assessment accreditation programme, and act on reports to improve the quality and safety of these processes.
Here we again saw big differences between countries, apparently quite independent of size, geographical location or economic status. The group found five countries showing more than 70% of hospitals undergoing external quality assessment, and three that have more than 80%, namely Slovenia, Romania and the Czech Republic (figure 11). Comments from several countries, for example, Ireland and Belgium, indicated that the implementation would be addressed in upcoming years. Some countries explained that they use internal quality assessment plans or they have regular certification inspections. The main barrier to implementation seemed to be the cost of providing external quality assessment service, together with the lack of availability of this in some countries.

S5.3: Percentage of negative responses per country.
Question S11 was asking about EAHP Statement 1.1: The overarching goal of the hospital pharmacy service is to optimise patient outcomes through working collaboratively within multidisciplinary teams in order to achieve the responsible use of medicines across all settings.
Given that the presence of pharmacists in healthcare multidisciplinary teams is considered indispensable for healthcare systems,5 the variation in the response to this question is remarkable, as shown in figure 12. The question S1.1 allowed for a broad definition of what is meant by ‘multidisciplinary team’. The responses demonstrate a correlation between the extent of clinical pharmacy services and compliance with this Statement.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
S1.1: Percentage of negative responses.
The responders repeatedly indicated that the main barriers were the imbalance in numbers of pharmacists and other healthcare professionals, lack of capacity or too big a workload or not actually being allowed to participate in multidisciplinary teams. Underpinning this was the impression that physicians did not think that hospital pharmacists had enough skills to fulfil certain tasks, or the hospital management was not willing to hire more hospital pharmacists to work in this role. The explanation for this might be hidden in fact that most countries (70%) reported hospital pharmacist roles were not explained in curricula of other healthcare professionals as emerged from the research made by EAHP via its annual country reports presented on General Assembly.
Discussion
This EAHP survey had certain limitations. One of the most important was its extent. While there are six sections with dozens of Statements, the survey group needed to keep the survey as short as possible in order to achieve a reasonable response rate. The authors sought a proper balance to get enough information to target EAHP's implementation well. However, the survey group could not easily quantify the main obstacles to implementation and most of the barriers were identified via qualitative research in free text responses. This was further complicated due to many language mutations the survey had been presented in. For few countries, the response rate was not high enough to make appropriate conclusions.4 Also, the level of awareness of Statements remains challenging in some countries, as discussed further in the article (pages 72–75).6
In spite of these limitations, the survey provided enough data to support and inform the EAHP implementation efforts. The Statements covering more traditional roles of hospital pharmacies, such as procurement of medicines, dispensing and compounding, were implemented to a higher extent than activities that became more recently part of hospital pharmacists’ competences portfolio, such as medication reconciliation. This seems to be related to the most frequently mentioned barrier in implementation of the Statement—limited capacity due to workload and insufficient staffing. While about 45% of hospital pharmacies serve hospitals with more than 500 beds (and about 90% to hospitals with more than 100 beds), a ‘typical’ hospital pharmacy (more than 70% of them) has less than 10 pharmacists. These numbers clearly prove that the capacity (which can be also translated to staffing and personal expenditures) is the most challenging issue deserving much attention. This is also related to the need to increase awareness about hospital pharmacists’ roles and competences among other healthcare professionals and hospital managers. Higher publication potential and wider active engagement in multidisciplinary education activities are probably also limited by insufficient capacity; however, greater publication outcomes also mean greater attention and awareness to our profession, leading to more frequent demands to engage hospital pharmacists in multidisciplinary teams in hospitals. This participation in hospital-wide processes is already implemented in terms of being part of hospital Drug and Therapeutic committees.
The authors believe that subsequent EAHP surveys dedicated more to quantification of the barriers of implementation will bring substantially more clarity to the main reasons why certain EAHP Statements remain under-implemented in some countries. These barriers may differ from country to country and from many of them there will be no single solution as to how to overcome them. For this purpose, the EAHP survey group provides national reports to our member associations containing all necessary data to plan further steps on national level.
Conclusion
The main objective of the EAHP baseline survey was to provide a baseline assessment of the level of implementation with the EAHP Statements throughout European countries. This enables the EAHP to prioritise efforts in our implementation activities. This objective has been reached, thanks to enormous effort of national coordinators and all our members who had responded to the survey. The data will now be used to inform the EAHP Statements implementation project, which is the subject of another paper.6
What this paper adds
What is already known on this subject
The European Statements of Hospital Pharmacy, expressing commonly agreed objectives which every European health system should aim for in the delivery of hospital pharmacy services, were prepared and approved in 2014.
No specific data describing the level of implementation and main barriers were present until now.
What this study adds
An overview of the level of the Statements implementation in the European Association of Hospital Pharmacists (EAHP) member countries.
Identification of the main barriers in the implementation.
Information to target EAHP implementation activities.
Acknowledgments
EAHP Survey Working Group: Leonidas Tzimis, Ercan Celikkayalar Adil and Vera Pires. Ms Jennie De Greef and EAHP staff. EAHP member association presidents and national survey coordinators.
Footnotes
Contributors PH, JP, JS, TMG and JU were involved in planning of the study, design of the questionnaire and conducting of survey. NG was involved in setting up the online form, along with respective language mutations. NG, JU and PH were involved in data evaluation and statistics. PH, JP and JU were involved in manuscript preparation.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.