Article Text

Abstract
Introduction This study investigates the drug selection and dispensing behaviour of hospital pharmacists of intravenous iron products including iron sucrose and iron sucrose similar, with special emphasis on substitution and interchangeability in France and Spain. Iron–carbohydrate complex drugs represent different available intravenous iron drugs and are part of the non-biological complex drug (NBCD) class, an expanding drug class with up to 30 brands available in intravenous pharmacotherapy and over 50 in clinical development. Follow-on versions of iron sucrose have appeared in some markets such as France and Spain, which were authorised by the generic approval pathway. However, differences in clinical efficacy and safety of iron sucrose similars compared with the reference originator drug Venofer have been observed, putting a question mark on their equivalence as assessed for authorisation and consequently their substitutability and interchangeability.
Method 70 French and 70 Spanish hospital pharmacists were surveyed via an online questionnaire on their formulary selection and dispensing behaviour of intravenous iron medicines.
Results There is little awareness about the characteristics of this class of drugs and the reported differences in safety and efficacy between iron sucrose and iron sucrose similars. In approximately 85% of cases the intravenous iron is chosen according to the hospital formulary. In 30% (France) and 34% (Spain) of cases an iron sucrose similar was dispensed because the formulary requires dispensing an alternative lower cost drug when available. In 26% (France) and 52% (Spain) of cases the physician is not informed on such a medication change using a similar product.
Conclusions Evaluation of NBCD similars for substitution and interchange by hospital pharmacists is rarely based on scientific and clinical criteria but rather on cost aspects only, which does not ensure safe, efficacious and cost-effective use of such drugs.
- non-biological complex drugs
- drug interchange
- intravenous iron
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
EAHP Statement 6: Education and Research
Introduction
Most intravenous iron products are used for the treatment of iron deficiency (anaemia). These complex drugs are nanomedicines that fall into the category of non-biological complex drugs (NBCDs). An NBCD is defined as “a medicinal product, not being a biological medicine, where the active substance is not a homo-molecular structure, but consists of different (closely related and often nanoparticulate) structures that can't be isolated and fully quantitated, characterised, and/or described by physicochemical analytical means. It is also unknown which structural elements might impact the therapeutic performance. The composition, quality, and in vivo performance of NBCDs are highly dependent on the manufacturing processes. Examples of NBCD are, amongst others, liposomes, iron–carbohydrate (‘iron–sugar’) drugs, and glatiramoids”.1 Although sharing a similar level of complexity to biologicals, this drug class is by definition different from biologicals and therefore is not assessed as such. Nevertheless, they share a similar paradigm. When follow-on iron sucrose products were developed, their colloidal/nanomedicinal aspect was not addressed and they were thus assessed according to the generic paradigm which was based on a sameness approach eventually granting therapeutic equivalence. Authorisation of generics is based on pharmaceutical equivalence showing the sameness of the active pharmaceutical ingredient and bioequivalence to the listed reference product, allowing efficacy and safety studies to be waivered. Generics are considered as interchangeable and substitutable copies, which means that pharmacists can repeatedly switch the originator to the generic with no obligation to inform the prescribing physician.
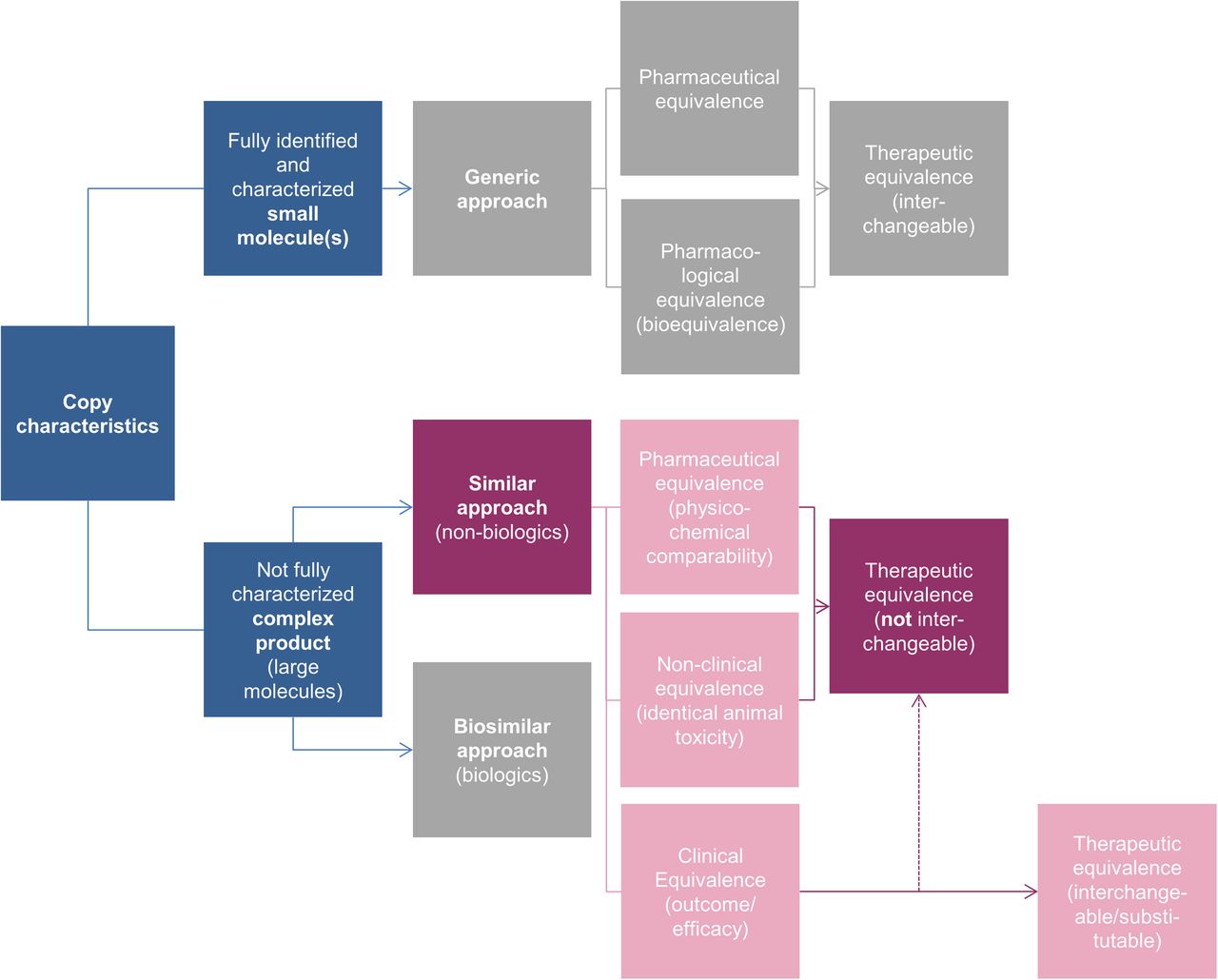
However, due to the complexity of NBCDs in structure and pharmacokinetics, showing equivalence is more challenging as the comparability evaluation deals with a physicochemically not fully identified/characterised high molecular drug entity (see figure 1). Also, the (active) uptake and distribution pattern, where the plasma drug concentration does not represent the pharmacologically driving central compartment, is not well understood. The uptake and biodistribution and, as a consequence, the pharmacodynamics are heavily dependent on the size/size distribution and composition of the nanoparticulate drug consisting of a polymeric core with a surrounding shell, which has implications on the kinetics, efficacy and safety of the drug. At present the clinically meaningful quality attributes remain unknown.

Reaching therapeutic equivalence for generics and similars.24
Two clinical studies in patients with late stage chronic kidney disease on haemodialysis demonstrated for the first time a lack of therapeutic equivalence for a nanosimilar (the originator Venofer) and its follow-on products.2 ,3 Venofer is a nanoparticulate iron sucrose preparation used intravenously to deliver iron (III) into the physiological iron pathway, often administered in combination with expensive erythropoietin stimulating agents (ESA) to achieve optimal haemoglobin (Hb) levels. Its follow-on products, so-called iron sucrose similars (ISS), were approved on a generic pathway without, for example, addressing particle sizing or biodistribution evaluation. The physicochemical and non-clinical comparative data of various ISS and the originator have been published in several studies. While some ISS are shown to be physicochemical and structurally similar to the originator, others are not even compliant with respective pharmacopoeia monographs.4–8 In two clinical studies, a rapid fall in Hb level and the related pharmacodynamic iron parameters such as ferritin and transferrin saturation (TSAT) were observed by substitution of the originator with an ISS. Significantly higher doses of intravenous iron as well as ESA were required for the ISS to stabilise the patients on the targeted Hb levels, making the use of an ISS also less cost-effective.2 ,3 It is noteworthy that the ISSs used were compliant with the pharmacopoeia requirements, suggesting that the critical clinically meaningful quality attributes of these types of medicinal products are not fully understood. Further clinical reports also showed different safety outcomes such as increased levels of inflammation markers in patients on haemodialysis and a significantly higher number of adverse events in gynaecology patients when using ISS.9 ,10 Notably, in at least two of these reports pharmacists substituted the originator drug with the follow-on version without giving notice to the prescribing physician, following common practice for generics but also presenting risks for best therapy practice and benefit for the patient. The clinical studies by Lee et al10 and Rottembourg et al2 were both investigator initiated studies supported by Vifor Pharma, while the clinical studies by Agüera et al3 and Martin-Malo et al9 were initiated independently by third parties.
The generic paradigm, lacking the specific clinical and non-clinical safety and efficacy data for the drug to be authorised, is not appropriate to assess follow-on NBCDs. Although ISS share the international non-proprietary name with the originator, it cannot be assumed that two formulations are therapeutically equivalent and therefore they can exhibit clinically meaningful differences. Repeatedly switching different formulations can pose problems for patients. Alarmed by these clinical findings, the US Food and Drug Administration and European Medicines Agency (EMA) have issued draft guidelines and reflection papers proposing stepwise in vitro, non-clinical and clinical testing as a prerequisite to define the extent of similarity and eventually the place in therapy, or the possibility of interchanging or switching between such products.11–14
Although the complexity of NBCDs and the consequences of showing therapeutic equivalence has been placed on the scientific agenda of regulators and regulatory scientists and is increasingly receiving attention, awareness still seems to be lacking among healthcare professionals, including hospital pharmacists who have to select such products for the hospital formulary and define their correct handling and use, directly impacting patients. In the case of NBCDs it is especially important that pharmacists take responsibility by using their pharmaceutical expertise in drug evaluation and selection to allow the right drug choice, aiming at therapeutic benefit for the patient and also the cost-effective use of drugs.
This study gives insight into the current decision-making process of pharmacists for the use of intravenous iron products in hospital and general practice and the perception of substitutability of different types of intravenous iron products including ISS as typical representatives of NBCDs.
Methods
A total of 140 hospital pharmacists involved in the evaluation and selection of formulary drugs in France and Spain (70 in each country) were surveyed via a 35 min online questionnaire in 2013. This number allows a confidence level of 90% and an error margin of 10%, assuming a number of 5000 hospital pharmacists practising in France and 3000 in Spain.15 ,16 They were screened based on the following key criteria: currently employed as a hospital pharmacist; practising for 3–30 years since completing formal pharmacist basic and specialised education and training; involved in drug purchasing decisions; and not affiliated as a clinical investigator, consultant, employee, speaker or in any other capacity with an advertising/marketing agency, marketing research agency, drug regulatory body or drug company. Other included criteria and numbers are shown in table 1.
Characteristics of the responding hospital pharmacists
Results
Awareness of differences between intravenous iron products
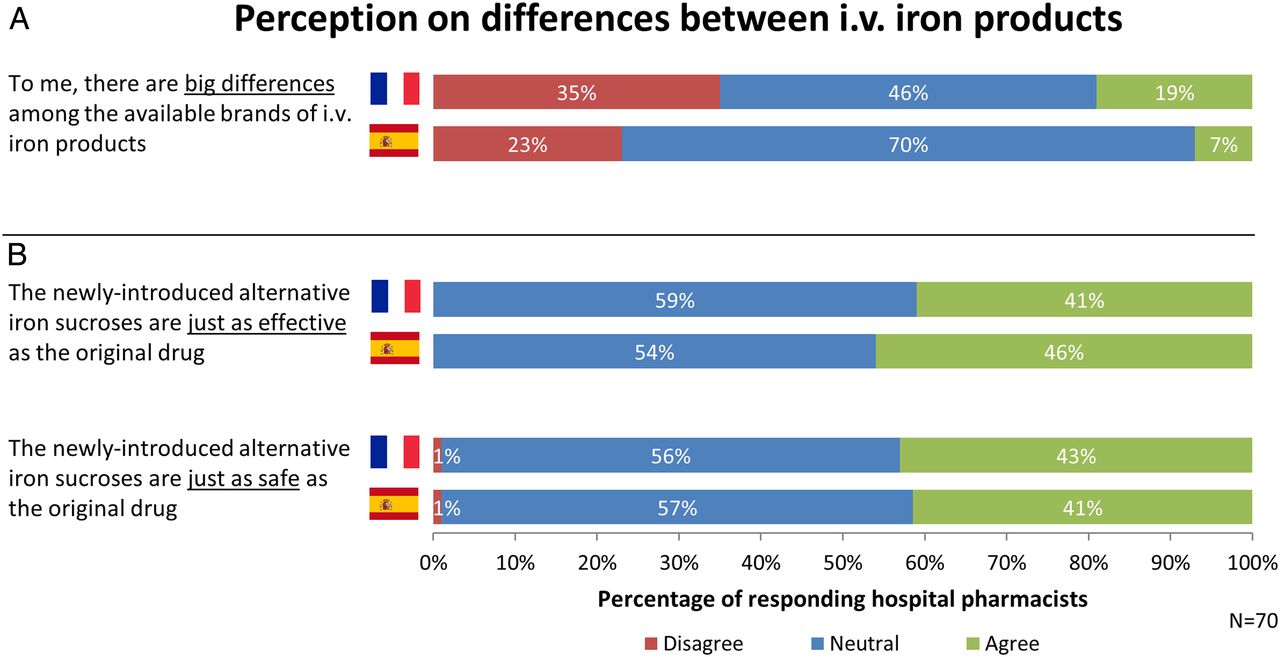
Awareness among hospital pharmacists of the differences between available originator intravenous iron brands is low. In France and Spain, 35% and 23% of hospital pharmacists, respectively, thought that there were no essential differences between available originator intravenous iron brands and only 19% and 7%, respectively, believed that there were important differences (figure 2A).
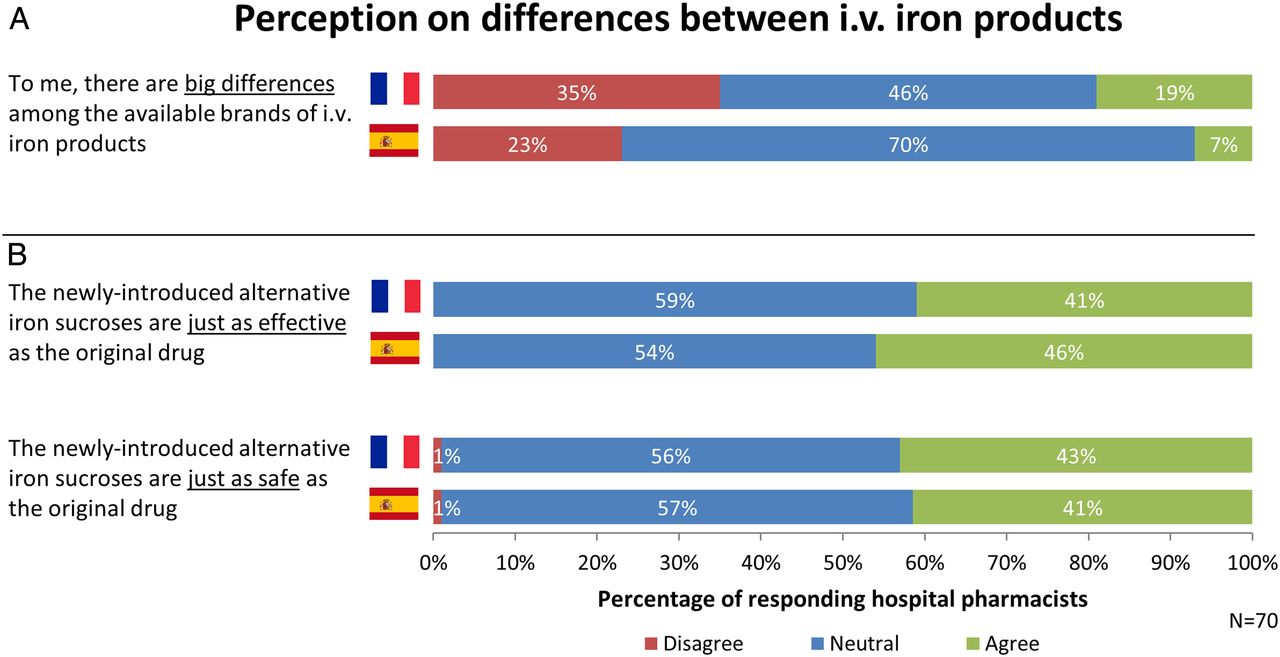
Results from the survey on pharmacists' perceptions of differences between available branded intravenous (i.v.) iron products (A) and between IS and iron sucrose similar (B) in 2013. A 7-point scale was used, where 1 stands for ‘completely disagree’ and 7 stands for ‘completely agree’.
For iron sucrose, a large proportion (±40%) of the hospital pharmacists indicated that ISS are just as effective and safe as the originator (figure 2B).
Substitution authority process
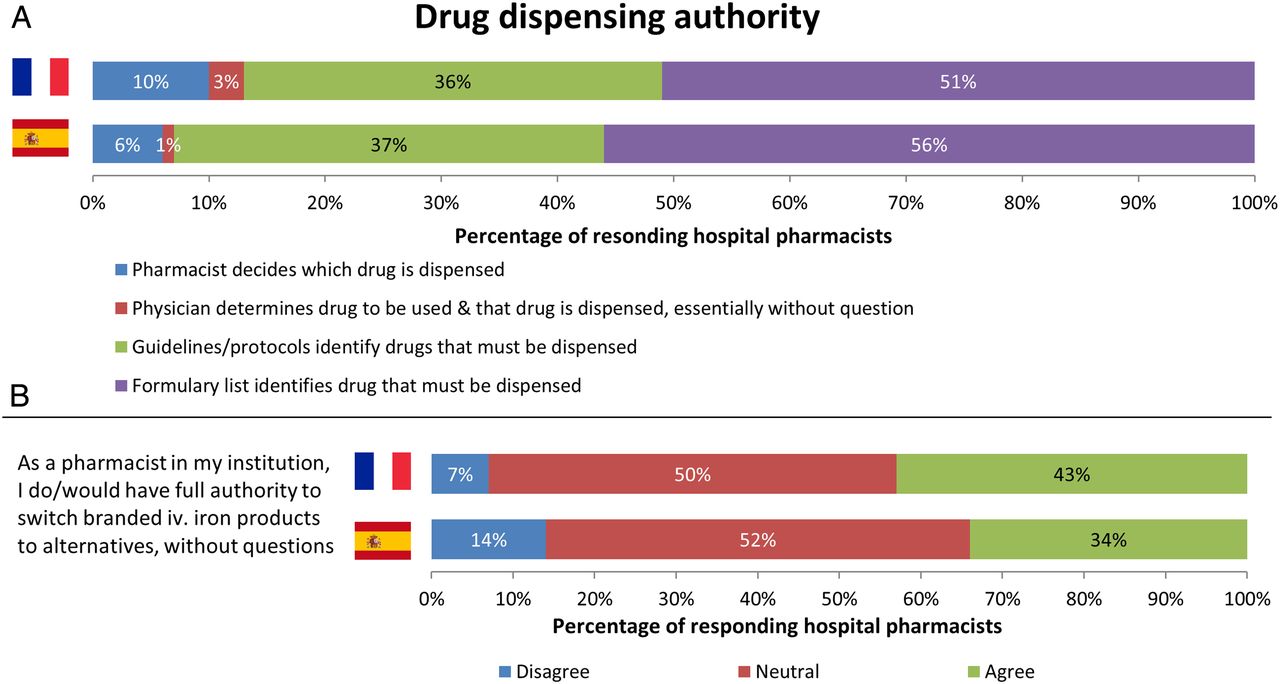
For drug dispensing, 80–90% of the decision on the use of a specific intravenous iron brand was made using the formulary list product or guidelines/protocols that direct drug dispensing (figure 3A). In the rest of the cases the decision on intravenous iron was made either by the physician or the pharmacist. As showed in figure 3B, 43% (France) and 34% (Spain) of the pharmacists mentioned that they have full authority to switch intravenous iron products to alternatives without questions.

Results from the survey on primary decision authority for intravenous (i.v.) iron product use (A) and the pharmacist's authority to switch branded iron to alternatives (B) in 2013. A 7-point scale was used, where 1 stands for ‘completely disagree’ and 7 stands for ‘completely agree’.
In the case of iron sucrose, 64% and 33% of the hospitals examined in France and Spain, respectively, did not include the IS originator on the formulary list. In France, the main reason for drug selection is the cost or coverage by the payer. 34% of the pharmacists perceived the cost/formulary coverage of an ISS as beneficial against 14% for the IS. 29% of the pharmacists saw the cost/formulary coverage restriction for the IS as a limitation while 9% saw this restriction for the ISS.
Who makes the actual decision?
According to figure 4A, the decision as to which iron sucrose to dispense is made by the prescribing physician in 27% (France) and 21% (Spain) of cases and by the pharmacist in 43% (France) and 45% (Spain) of cases. In the remaining 30% and 34% of cases the pharmacist is obliged to dispense an ISS according to the institution's standard operating procedures to use a ‘cheaper’ alternative when available.

Results from the survey on decision-making behaviour for dispensing alternative iron sucrose drugs (A). The blue rods together represent the proportion where the decision to dispense an iron sucrose similar (ISS) is made by the physician (27% in France, 21% in Spain). The green rods together represent the proportion where the decision to dispense an ISS is made by the pharmacist (43% in France, 45% in Spain). The red rods represent cases where pharmacists are required to dispense an ISS (30% in France, 34% in Spain). (B) Behaviour of pharmacists of informing physicians when they decide to switch to an alternative iron sucrose drug in 2013. The proportion of physicians not informed is the sum of answers 4+5+7 from figure 3A and the proportion of physicians informed is the sum of answers 1+2+3+6 from figure 3A.
When the hospital pharmacist is allowed to dispense an alternative iron sucrose drug, the prescribing physician is in most cases informed as a courtesy (figure 4A). In France and Spain, 74% and 48% of the pharmacists, respectively, inform the prescribing physician about dispensing an ISS while 26% and 52% of the pharmacists, respectively, do not inform the prescribing physician (figure 4B).
Consequences of current dispensing behaviour
The decision taken in hospitals regarding dispensing iron sucrose upon prescription has resulted in an average of 47% and 38% substitution of the branded IS into an ISS within different wards in France and Spain, respectively (figure 5). This number has changed in an inconsistent way compared with 2012. In some wards the use of ISS has increased while in others it has decreased.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results from the survey on the average frequency (%) an iron sucrose similar (ISS) is dispensed instead of an iron sucrose drug in various wards in France (left) and Spain (right) in 2012 and 2013. N stands for the number of hospital pharmacists that responded the question.
Discussion
Different originator brands of intravenous iron products composed of measurably different iron carbohydrate complexes show differences in clinical efficacy and safety profiles. This leads to individual labels with respect to posology and safety profiles, for example, as they are not identical and interchange and substitution should not even be considered.17–21 Despite this fact, many pharmacists are not aware of important differences among different originator brands of colloidal intravenous iron products representing nanomedicines. We did not investigate whether different originator intravenous iron products are interchanged in the clinics.
ISS, follow-on versions of the originator Venofer, share the international non-proprietary name. They were approved in the past in France and Spain like generics based on therapeutic equivalence to the listed reference product Venofer, suggesting equivalence and therefore substitutability. For biosimilars, another class of complex drugs with an established approach for approval ahead of their entry into the market, automatic substitution is not recommended by the EMA. Recent studies after approval of ISS have shown decreased control of key outcome pharmacodynamic parameters in iron deficiency anaemia therapy such as Hb levels and TSAT when switching from the originator iron sucrose to an ISS.2 ,3 This triggered a discussion in the regulatory science community and by widely accepted authorities on how to improve the approval standards for nanomedicines and NBCDs such as intravenous iron products to safeguard efficacy and safety in patients.11–14 In many countries, ISS are on the market approved in the past as generics but, with today's knowledge, they should not be considered substitutable.2 ,3 Therefore the pharmacist, based on his specific knowledge of drug products, has an important role in the evaluation of the interchangeability and substitutability of these medicinal products to ensure safe and efficacious use of intravenous iron and other NBCDs in the hospital. This survey shows that there is a lack of awareness among hospital pharmacists regarding the specific characteristics of NBCDs and their nanosimilars which translates into efficacy and safety differences observed and published, especially for iron sucrose, a widely accepted standard for intravenous iron therapy, and the ISS. As a consequence, these follow-on products are frequently used in all relevant hospital wards based on an abbreviated decision-making process suitable only for fully substitutable generics but not for nanosimilars.
The choice of drug is primarily given by a restrictive drug formulary list. This list is a result of a drug selection process and is the basis for guidelines on how to use drugs including rules on interchangeability. Pharmacists have the power to freely substitute a branded originator and alternative products where therapeutic equivalence is granted within their institute. This should not apply for intravenous iron colloidals, given the similarity approach. In addition, ISS substitution by the pharmacist frequently occurs without consulting or informing the prescribing physician, which is not an appropriate pharmaceutical standard and could give rise to concerns about therapeutic failure and prolonged periods of inadequate treatment. Moreover, it can result in pharmacoeconomic loss. This is in contrast to available guidance on criteria for evaluating biosimilars in formulary decisions—for example, the System of Objective Judgment Analysis (SOJA) method22 ,23—as no such guiding principles have so far been published for NBCDs or nanomedicines. There is currently no awareness of or education on the limits of interchange and substitution of complex drugs.
Conclusion
This study shows the limited awareness among hospital pharmacists about possible clinical differences between NBCDs and their follow-on similars. To improve patient benefit and cost-efficient treatment with NBCDs such as intravenous irons, appropriate understanding and knowledge has to be provided. Furthermore, evaluation tools, guidelines and continuous medical education programmes must be implemented to ensure correct decisions regarding drug selection, interchange and substitution are made based on scientific and clinical data. Hospital pharmacists are key in drug evaluation and selection for the drug hospital formulary and related guidelines and instructions regarding substitution and interchange among similar products or therapeutic alternatives. At present there is no established or harmonised regulatory approval process in the context of NBCDs. It is therefore important that pharmacists are educated to fill the gap with their expertise to evaluate these drugs in a systematic, scientific and data-based manner in order to ensure safe, efficacious and cost-effective use.
What this paper adds
What is already known on this subject
Nanosimilars approved by the generic pathway have been shown to be clinically different.
It is not known how healthcare professionals use nanosimilars regarding interchange and substitution.
What this study adds
This study shows that the knowledge about potential clinical differences between nanosimilars, using colloidal intravenous iron as a representative, is very limited among French and Spanish hospital pharmacists.
The consequence is that nanosimilars are often seen and used as generics regarding interchange and substitution.
References
Supplementary materials
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Funding This paper is funded and commissioned by Vifor Pharma.
Disclaimer Data were derived by Ipsos, contracted by Vifor Pharma.
Competing interests JK, BF and SM are employed by Vifor Pharma, the market authorisation holder of intravenous iron products Venofer and Ferinject.
Provenance and peer review Not commissioned; externally peer reviewed.