Article Text

Abstract
Objectives Hospital admission rates for hypoglycaemia now exceed those for hyperglycaemias among older adults. A growing number of reports associating hypoglycaemia with non-antidiabetic drugs have been published. Clinical pharmacists are often faced with hypoglycaemia in patients taking multiple medications. This study assessed the potential relationship between prescribed drugs and episodes of hypoglycaemia during hospitalisation.
Methods Point-of-care blood glucose values and prescribed drugs were analysed in patients admitted to a regional hospital. Hypoglycaemia cases were defined as patients with at least one hypoglycaemic event (random glucose value ≤3.9 mmol/L), and normoglycaemic cases as those with random glucose concentrations within the range of 4.5–5.8 mmol/L. Analyses were carried out using multivariate logistic regressions and Cox proportional hazard models.
Results 373 patients (53% males; median age=74 years) were included in the analysis and of these, 64 (17%) had at least one hypoglycaemic event. Patients who experienced a hypoglycaemic event had a longer length of stay (median=10 vs 7 days, p<0.01) and a higher rate of antidiabetic drugs prescription (83% vs 37%, p<0.01). The number of non-antidiabetic drugs was associated with an increased risk of hypoglycaemia during hospitalisation (HR 2.3, 95% CI 1.4 to 4, p<0.01). After adjusting by confounders, heparin and pantoprazole were found to be associated with hypoglycaemia.
Conclusions The relationship between hypoglycaemia and polypharmacy reinforces the advice to limit polymedication as much as possible, especially in elderly patients. This result underlines the potential involvement of clinical pharmacists with the aim to reduce the risk of hypoglycaemia during hospitalisation.
- clinical pharmacology
- diabetes & endocrinology
- internal medicine
- side effects of drugs
- geriatric medicine
Statistics from Altmetric.com
- clinical pharmacology
- diabetes & endocrinology
- internal medicine
- side effects of drugs
- geriatric medicine
Introduction
Concerns about hypoglycaemia have been raised since the publication of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study showing an increase in mortality in the intensive glucose treatment arm.1 The incidence of hypoglycaemia in hospitalised patients in the USA ranges from 3.5% to 10.5% in patients without diabetes2 3 and up to 23% in patients with diabetes.4 5 It is of note that the definition of hypoglycaemia is subject of debate, mainly because the relationship between glucose levels and symptoms is highly variable between subjects and depends on characteristics such as age and duration of diabetes.6 7 The American Diabetes Association (ADA) has proposed a threshold of hypoglycaemia at 3.9 mmol/L, although symptoms may occur above this concentration in poorly controlled patients with diabetes or lower in elderly patients.8 9 Since hypoglycaemic events during hospitalisation are associated with a prolonged stay and increased costs,2 10 11 detection of at-risk patients is of major importance. In terms of prognosis, spontaneous hypoglycaemia can be distinguished from iatrogenic hypoglycaemia. Spontaneous hypoglycaemia is often observed in critically ill patients and is associated with severe illnesses such as septic shock or acute renal failure.12 13 It would be partly explained by an alteration of hormonal responses to decreased blood glucose levels. The most common risk factor for iatrogenic hypoglycaemia in hospitalised patients is the use of glucose-lowering agents such as insulin therapy.14 The incidence of hypoglycaemia is strongly related to insulin use, with an incidence of mild hypoglycaemic (defined as self-treated hypoglycaemia) episodes of 2.7 per person-year among patients with type 2 diabetes and 13.7 per person-year among patients with type 1 diabetes.15 The duration of insulin therapy is also related to the frequency of hypoglycaemic events in type 2 diabetes mellitus, which could be partly due to decline of pancreatic β cell functions.16 Insulin secretagogues such as sulfonylureas (eg, glimepiride, glibenclamide) or meglitinides (eg, nateglinide, repaglinide) are also known to induce hypoglycaemic events. Whereas this adverse effect is expected for antidiabetic drugs, reports describing reduction of blood glucose concentration by other drugs are emerging, mostly based on low-quality evidence. Moreover, the underlying pharmacological mechanisms are often unknown or poorly understood. Among these drugs, several antibiotics have been associated with hypoglycaemia. For example, cases of hypoglycaemia due to sulfamethoxazole–trimethoprim have been published. They mostly occur in patients with renal failure, underlining the necessity of dose reduction in this population.17 18 Furthermore, co-prescription of sulfamethoxazole–trimethoprim with an insulin secretagogue such as glipizide or repaglinide would increase the risk of hypoglycaemia.17 19 Other antibiotics such as quinolones (eg, ciprofloxacin, gatifloxacin, levofloxacin and moxifloxacin) are also described as inducing dysglycaemia with a different rate depending on the molecule.20 According to Park-Willye, gatifloxacin was strongly associated to hypoglycemia-related hospital admission of elderly patients, followed by levofloxacin. In contrast, moxifloxacin and ciprofloxacin were not associated with hypoglycaemia.21 To date, quinolone-induced hypoglycaemia remains a matter of debate.22 ACE inhibitors or β-blockers are also suspected to be associated with hypoglycaemia, particularly in patients with diabetes. Hypoglycaemia related to ACE inhibitors is debated due to conflicting results from cohort studies.23 24 However, significant effects have been observed in patients with diabetes compared with patients without diabetes, suggesting a synergistic effect between diabetes and ACE inhibitors or possible drug interactions between antidiabetic drugs and ACE inhibitors.24 25 By interfering with adrenergic counter regulation, β-blockers are suspected to mask hypoglycaemic clinical signs, despite conflicting results.26 Other drugs have been reported to cause hypoglycaemia in patients without diabetes as shown by cases depicted in online Supplementary table 1.
Supplementary file 1
Of note, drug–drug interactions could be part of the underlying mechanism of drug-induced hypoglycaemia. For example, common anti-infective drugs such as azoles, quinolones, macrolides and sulfonamides were reported to be associated with a decrease of glycaemia when they were associated with glipizide or glyburide.27 Polymedication predisposes patients to drug–drug interactions. Elderly patients are particularly concerned. Moreover, as shown by the ACCORD study, hypoglycaemia symptoms occurs more frequently in elderly patients underlining that this population needs a special attention.28
Due to the clinical importance of this side effect, recognising which agents can induce or worsen hypoglycaemia is of major clinical relevance. The present study aims to identify medications associated with hypoglycaemic episodes in inpatients of a Swiss regional hospital. The effects of age and gender, as well as co-administration of antidiabetic drugs and polymedication, were also investigated.
Methods
Setting and design
A nested case–control design was used to examine the association between drug use and hypoglycaemia. Data from adult patients admitted to internal medicine, orthopaedics, gynaecology/obstetrics or private wards from January 2013 to December 2015 were analysed. Of note, the private unit is a mixed ward with patients of these three medical specialties. As the study design was non-interventional and retrospective, and patients’ identity was masked, no informed consent was required.
Sources of data and database creation
Blood glucose values, sampling time and date, age and gender were extracted from the in-house medical analysis laboratory database. Capillary blood samples were analysed with a point-of-care system (Accu-Check Inform II, Roche Diagnostics, Basel, Switzerland). Venous glycaemic values were processed on a Beckman-Coulter DXC660 platform (Beckman Coulter, Galway, Ireland). Prescribed drugs, date of drug intake, administration route, dosage, validation of drug delivery, admission and discharge date were extracted from healthcare information records (PrediMed, Lausanne University Hospital, Switzerland). Drugs for topical use, laxatives and ophthalmic drugs were excluded from analysis. For simplification purposes, multiple drug intakes per day were considered to be one intake per day and drug dosages were not considered. Both data sets were linked together using patients’ identity number, while the dates when blood samples were taken were matched with the date of drug intake. Patients’ identity number were then replaced with random codes and the algorithm destroyed before data were received for analysis. Observations with missing data were excluded from further analysis. For patients with multiple admissions, only the first admission was included in the analysis.
Hypoglycaemic and normoglycaemic group
The hypoglycaemic group was defined as all patients having at least one random glucose value equal to or lower than 3.9 mmol/L according to the ADA and The Endocrine Society.29 Patients with normoglycaemia were defined as patients with all random glucose values ranging from 4.5 to 5.8 mmol/L. To increase specificity between the two groups, patients with random glucose ranging from 4.0 to 4.5 mmol/L were not considered for analysis.
Statistical analysis
Descriptive statistics were made by presenting median and 25 and 75 percentiles for continuous variables and numbers and percentages for categorical variables. Marginal analysis were made by using Fisher’s exact test for categorical variables and Mann-Whitney tests for continuous variables. Both tests were two-sided, with p values ≤0.05 considered as statistically significant. Cox proportional hazards models and Kaplan-Meier analysis were used to assess the first event of hypoglycaemia during hospitalisation.
Fisher’s exact tests were used to investigate the associations between drugs and the hypoglycaemic events. Significant associations (p values ≤0.05) were confirmed by logistic multivariate models, which included available confounding factors. All statistical analyses were carried out using R software (The R foundation, www.r-project.org, V.3.3.1).
Results
Demographic
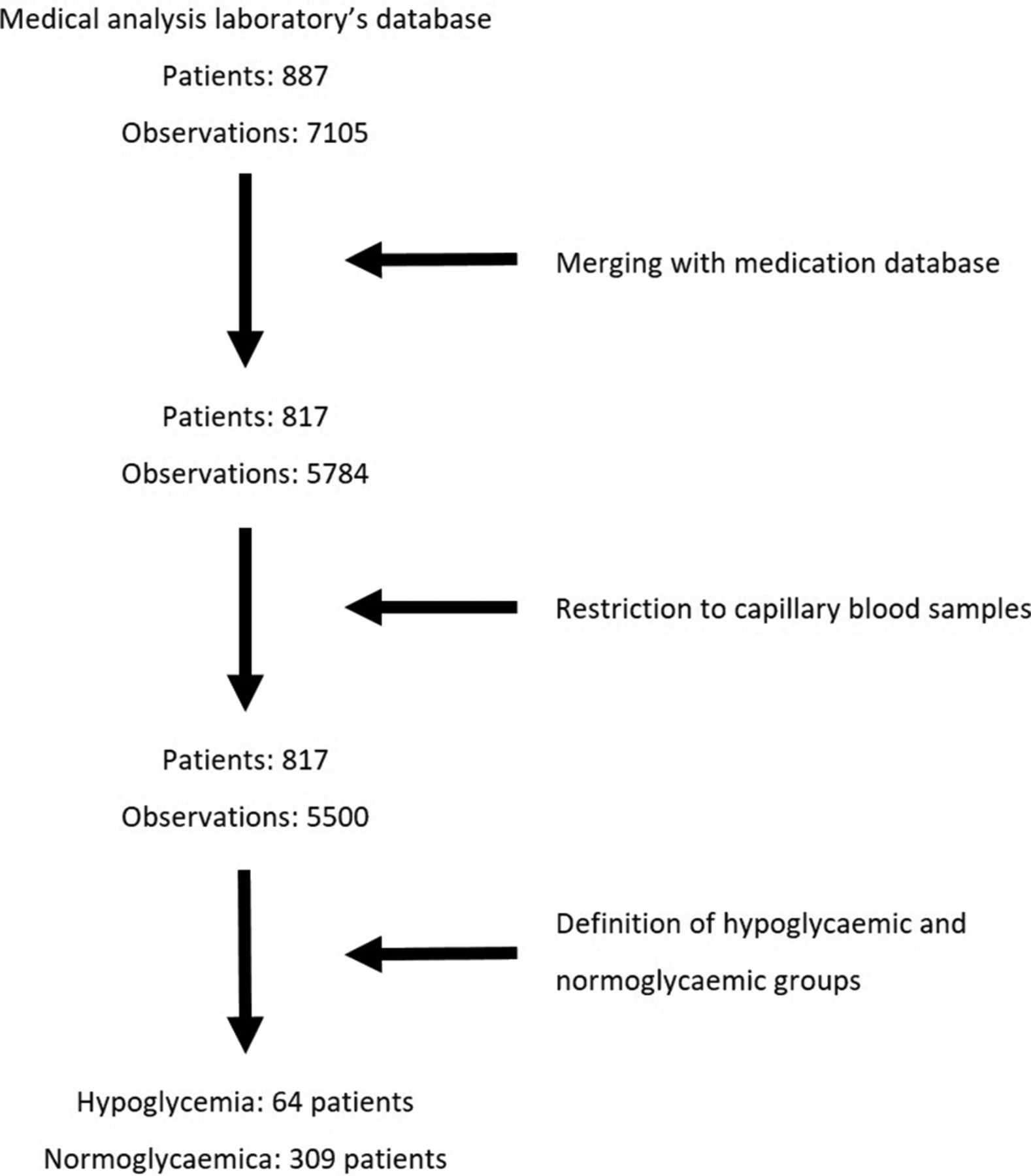
Seven thousand one hundred and five glucose values representing 887 patients were extracted. These figures were reduced to 5500 glucose values, representing 817 patients after merging with the medication database and only retaining capillary blood samples (see figure 1 for more details). Furthermore, 373 patients were retained for analysis, of whom 92 (25%) were hospitalised in the orthopaedics department, 184 (49%) in the internal medicine department, 17 (5%) in gynaecology/obstetrics and 80 (21%) in the private unit. Age, gender, number of glycaemic analysis and the amounts of drugs were found to be significantly different between the four medical departments, explained in part by the demographic specificities of the gynaecology ward (see online Supplementary table 2). The prevalence of hypoglycaemia was similarly observed among the four medical wards, allowing these data to be combined for further analysis.
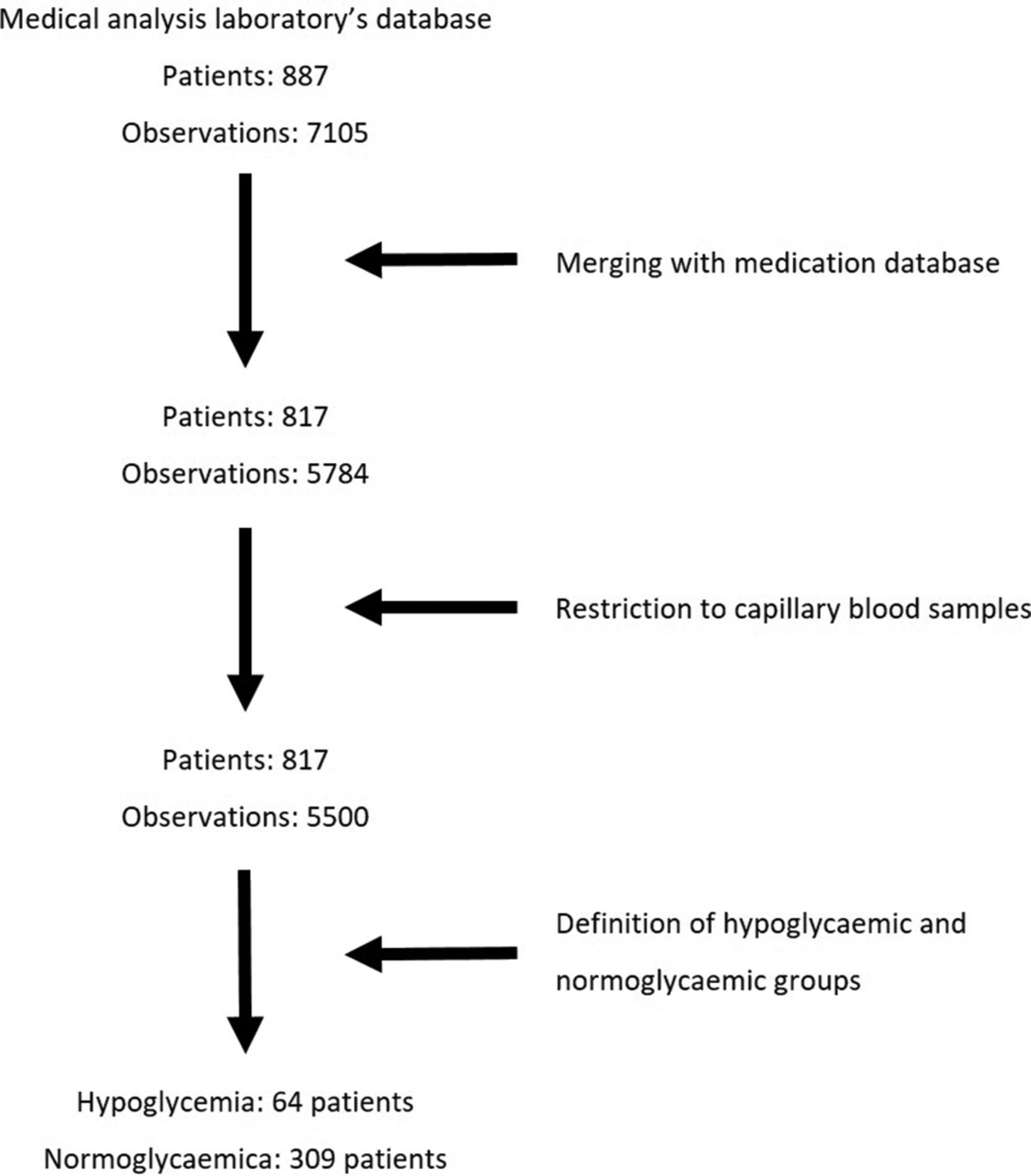
Study flow chart.
As shown in table 1, the proportion of males and median ages were found to be similar among patients with normoglycaemia and hypoglycaemia. The latter had more drugs prescribed per day and a longer hospitalisation stay than patients with normoglycaemia (median number of prescribed drugs 12 vs 9, p<0.001; median hospitalisation stay 10 vs 7 days, p<0.001). The proportion of patients with antidiabetic drugs was found to be higher in the hypoglycaemic group than in the normoglycaemic one (83% vs 37%, p<0.001). Patients with hypoglycaemia had more glycaemic controls than patients with normoglycaemia (13 vs 3, p<0.001). Among patients with hypoglycaemia (table 2), the first hypoglycaemic event occurs after a median of 4 days of hospitalisation and 30 patients (47%) had two or more hypoglycaemic events during their hospitalisation. Although not significant, the number of prescribed drugs tends to be lower in patients with one hypoglycaemic event than in patients with more events.
Comparison between patients with normoglycaemia and hypoglycaemia
Comparison between patients with one hypoglycaemic event and more or equal than two events
Drugs associated with hypoglycaemia
More than 340 different drugs were found in the analysed sample, with paracetamol, pantoprazole and enoxaparin being the most prescribed drugs (63.3%, 49.6% and 43.8%, respectively). As described in table 3, the use of fast-acting and medium-acting insulin was found to be significantly associated with hypoglycaemia (OR 8.4, p<0.001 and OR 11.1, p<0.001, respectively). The use of insulin secretagogues was also significantly associated with hypoglycaemia (sulfonylureas: OR 2.6, 95% CI 0.9 to 6.8, p=0.05; glinides: OR 15, 95% CI 1.2 to 793, p=0.02). The use of other antidiabetics, such as metformin, inhibitors of dipeptidyl peptidase-4 (DPP-4) or glucagon-like peptide-1 (GLP-1) receptor agonists, was not found to be associated with hypoglycaemia. Of note, six patients (2%) had a three-drug regimen (insulin plus insulin secretagogues plus another antidiabetic), among them two presented hypoglycaemic events. The strongest associations between non-antidiabetic drugs and hypoglycaemia are presented in online Supplementary table 3. The most significant results were observed regarding heparin, torsemide and tacrolimus. These significant associations were further analysed using a logistic multivariate model, with regard, for example, to insulin and/or insulin secretagogues use, age and gender. Heparin and pantoprazole remained significantly associated, even after adjusting for available confounders (see online Supplementary table 4).
Comparison of antidiabetic drugs between normoglycaemic and hypoglycaemic groups
Polymedication and hypoglycaemia
After excluding antidiabetic drugs, the median number of eight drugs per day was found in the analysed cohort. Patients with hypoglycaemia had a higher number of prescribed drugs than patients with normoglycaemia (10 vs 8, p<0.001). As shown in table 4, patients with more than eight prescribed drugs per day (178 patients) were older and had a longer hospitalisation stay than patients with eight or fewer prescribed drugs (76 vs 71 years, p=0.002; 8 vs 7 days, p=0.003). Furthermore, patients with more than one hypoglycaemic events were more frequently observed in the group of patients with more than eight prescribed drugs (13.5% vs 3%, p<0.001). Kaplan-Meier survival curves indicated a higher rate of hypoglycaemia among patients with more than eight prescribed drugs per day (figure 2). Cox proportional hazard models confirmed a significantly higher rate of hypoglycaemia during hospitalisation among patients with more than eight prescribed non-antidiabetic drugs per day, even after adjusting for hospitalisation duration, age and gender (adjusted HR 2.3, 95% CI 1.4 to 4, p=0.002) .
Comparison of patients with less or equal than eight non-antidiabetic drugs use and more than eight drugs

{kind=link}
{kind=link}
Polymedication and hypoglycaemic events during hospitalisation. The green Kaplan-Meier curve represents the patients with less than or equal to eight non-antidiabetic drugs per day, and the blue curve represents patients with more than eight drugs per day.
Discussion
We aimed to investigate whether non-antidiabetic drugs were associated with a hypoglycaemia event during hospitalisation. In the cohort containing all patients, a prevalence of 7.8% (64/817) of hypoglycaemia events was observed, which ranges close to previous published data.2 3 A higher prevalence of hypoglycaemia ranging from 12% to 18% was reported in patients with diabetes.4 This difference could be explained by the fact that the present cohort includes not only patients with diabetes but also non-diabetic ones. Although no specific geriatric ward was included in the present study, a median age of 74 years was observed. Thus, our results could be interpreted from a geriatric perspective rather than the view of an adult population.
Elderly patients are at high risk for hypoglycaemia due in part to reduced awareness of symptoms and to an altered physiological response, probably explained by an impaired counter-regulatory response to hypoglycaemia.30 31 Moreover, the presence of multiple chronic illnesses, which is of particular concern in this population, is a contributing factor for hypoglycaemic events independently of the diabetic status.2 Comorbidities expose patients to polymedication and, thus, to an increased risk of drug–drug interactions and adverse events.32 In the present study, we found an association between the number of prescribed non-antidiabetic drugs and hypoglycaemia (a threshold of eight drugs was used according to the median number of non-antidiabetic drugs). This association remained significant after adjusting for age, gender, hospital length of stay and antidiabetic drug use. This result is in line with the previous studies pointing out that elderly patients with diabetes with more than 4–5 medications per day were at risk for hypoglycaemia.33 34 Of note, in our study, the association between more than four drugs and hypoglycaemia events was also significant (data not shown). To our knowledge, no data is published about polymedication and hypoglycaemia in patients without diabetes, except for a study in elderly patients investigating unplanned hospitalisations due to adverse events. The authors found that hypoglycaemia was the second cause of admission after bradycardia stressing the impact of polymedication.35 Hypoglycaemia induced by polymedication can be explained, in part, by the increased risk of drug interactions. For example, co-prescription of sulfonylureas and quinolones or sulfamethoxazole–trimethoprim were associated with hypoglycaemia in elderly patients,36 as well as non-cardioselective β-blockers by masking hypoglycaemia symptoms during insulin therapy.37 In our cohort, no specific interaction was found to be associated with hypoglycaemia, explained in part by the broad range of different drugs and thus reducing statistical power.
After adjusting for available confounders, the use of heparin and pantoprazole remained significantly associated with hypoglycaemia. To our knowledge, only one report described a hypoglycaemic event during heparin treatment in a 63-year-old patient after adding heparin to glipizide. The authors suspected a displacement of the bound fraction of glipizide by an indirect increase of free fatty acids following heparin administration.38 This hypothesis could not be observed in the present cohort since no hypoglycaemic cases during heparin treatment with sulfonylureas were found. As enoxaparin is commonly used for antithrombotic prophylaxis and replaced by heparin in case of renal failure, we can hypothesise that there are more cases of renal failure in the heparin group. Renal function could not be obtained in the present study. However, by considering age as a good proxy for renal function decrease, patients treated with heparin were found to be older than patients treated by enoxaparin (data not shown), supporting our hypothesis. Renal failure is known to induce hypoglycaemia by decreasing renal gluconeogenesis or clearance of some antidiabetic drugs.39 Thus, further studies are needed to better define the impact of heparin itself on hypoglycaemia.
Only one pharmacovigilance study on pantoprazole mentions hypoglycaemia but without giving any precision.40 Interestingly, patients exposed to proton pump inhibitors (PPIs) have approximately 0.5% lower glycosylated haemoglobin values than unexposed patients.41–44 Moreover, recent data have shown that patients with upper gastrointestinal disease exposed to PPIs for 5 years have a lower risk of developing type 2 diabetes.45 An improvement of beta cells’ function after a 12 weeks PPI treatment of patients with and without diabetes suggests a potential protective role in glucose homeostasis.46 Besides, a possible effect on glycaemic parameters, this mentioned hypothesis cannot explain a spontaneous hypoglycaemia.
Several limitations of the present study need to be acknowledged. First, the glycaemic values were retrospectively collected exposing this study to a potential selection bias of cases who have a suspicion of altered glucose metabolism, resulting in an over-representation of patients with known glucose-related disorders. Second, the absence of covariates such as clinical parameters or diagnostic is of major concern. In the present study, we cannot rule out that the number of prescribed drugs is a marker of comorbidities and/or disease severity. Thus, this finding can be related to an elevated number of comorbidities and/or disease severity and not to the number of prescribed medications. To address this limitation, we adjusted the analysis by the hospitalisation duration which may be considered a proxy of illness severity.47 Third, the observational and non-interventional setting of this study will produce a broad number of drugs with, consequently, low statistical power. Except for PPIs, no significant association were observed after clustering drugs together regarding their pharmacological category. A strength of the present study in the naturalistic setting is giving a good overview of hypoglycaemia prevalence during hospitalisation.
Conclusion
This study explores the potential role of drugs to induce hypoglycaemia during hospitalisation, showing that heparin and pantoprazole might be associated with hypoglycaemic events. These observations need to be confirmed in independent studies. The relation between hypoglycaemia and the number of prescribed drugs supports the necessity to limit polymedication as much as possible especially in elderly patients. This goal can be achieved only by considering approaches such as relating each medication to the current disease.
What this paper adds
What is already known on this subject
Hospital admission rates for hypoglycaemia now exceed those for hyperglycaemia among older adults.
A growing number of reports associating hypoglycaemia with non-antidiabetic drugs have been published.
What this study adds
An association between hypoglycaemia events and the number of prescribed non-diabetic drugs during hospitalisation was found.
This observation reinforces the advice to limit polymedication as much as possible, especially in elderly patients.
Acknowledgments
The authors are grateful to Cazorla Christophe for his implication in collecting data.
References
Footnotes
EAHP Statement 4: Clinical Pharmacy Services.
Contributors FV and NS contributed to the conception and design of the study. FV and MM were responsible for the acquisition of data. FV, CC and NS were involved in the analysis and interpretation. FV drafted the manuscript and did the statistical analysis. NS obtained funding for the study. All authors contributed to the critical revision of the manuscript for important intellectual content and administrative, technical, or material support.
Funding This work has been funded by the Pharmacie Interhospitalière de la Côte, Morges, Switzerland. The funding sources had no role in the writing of the manuscript or in the decision to submit it for publication.
Competing interests None declared.
Ethics approval Local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.