Article Text

Statistics from Altmetric.com
- chromatography, high pressure liquid
- vancomycin hydrochloride
- drug stability-indicating method
- infusion, intravenous
- particulate contamination
Introduction
Vancomycin hydrochloride is an antibiotic belonging to the glycopeptide family and acts by inhibiting the synthesis of the peptidoglycan wall. This antibiotic is active against Gram-positive aerobic and anaerobic bacteria1 2 and is commonly used in hospitals to treat serious infections.3 4
Vancomycin has slow bactericidal time-dependent activity and can be administered by continuous or intermittent intravenous infusion. In France, administering vancomycin by continuous infusion over 24 hours is recommended.5 6
The Summary of Product Characteristics (SmPC) recommends reconstituting a 1 g vial with 20 mL of water for injection (WFI), then diluting it in 100 mL of saline solution. The amount of vancomycin to treat an adult infection is superior to 1 g and so the volume administered can be higher than 100 mL. This volume must be limited in children or in patients on water restriction, such as those suffering from hyponatraemia and cardiovascular diseases or are in intensive care.7
Some studies on vancomycin stability have already been performed. Solutions at 5 and 10 mg/mL were stable for 58 days at +4°C in 100 mL polyvinyl chloride (PVC) infusion bags with no specification with regard to protection from light.8 Vancomycin was stable at 5 mg/mL in PVC bags for 48 hours at +22°C without protection from light and for 7 days at +4°C with protection from light.9 Raverdy et al 10 examined the stability of vancomycin diluted in 5% dextrose at high concentration (83 mg/mL) and was stable for 72 hours at +37°C.
However, none of these studies reflects real infusion conditions as vancomycin is usually administered at 30 mg/kg/day.11 12 In practice, clinical services infuse vancomycin into electric syringe pumps using 50 mL (for adults) or 20 mL (for children) syringes. No stability study has yet been performed for such concentrations, in 50 or 20 mL syringes, at room temperature, nor has the reconstitution procedure13 been assessed. SmPC recommends reconstitution in WFI, then dilution in saline solution. However, in clinical units, vancomycin is often reconstituted and diluted in saline solution.
The aim of this work was therefore to study vancomycin stability in syringes and assess its use (pH, osmolality, number of particles) during a continuous 24-hour infusion with and without inline filters at four concentrations—25, 40, 60 and 80 mg/mL—reconstituted in two solvents (WFI and saline solution) and diluted in saline solution.
Materials and methods
Chemicals
The commercialised vancomycin used in this study came in lyophilised powder form (500 mg or 1 g vancomycin hydrochloride with the following excipients: mannitol, 0.5 N sodium hydroxide and 0.5 N hydrochloric acid) from Sandoz (Levallois-Perret, France). Vancomycin was reconstituted with WFI (Baxter, Guyancourt, France) or saline solution (0.9% sodium chloride; Baxter) and diluted in the same saline solution. European Pharmacopoeia (EP) standard vancomycin powder (Code: V0045000, Council of Europe, Strasbourg, France) was used to validate the assay method in WFI to reach a vancomycin concentration of 400 µg/mL. To perform the mobile phase, acetonitrile (high-performance liquid chromatography (HPLC) gradient grade; VWR Chemicals, Fontenay-sous-Bois, France), phosphate buffer (potassium dihydrogen phosphate; Merck, Calais, France), ultrapure water (Purelab Classic Elga System, Veolia, Wasquehal, France) and orthophosphoric acid (Merck) were used.
For the degradation protocol, 35% hydrochloric acid (Merck), 37% sodium hydroxide (VWR Chemicals) and 1% hydrogen peroxide (Gilbert, Hérouville-Saint-Clair, France) were used.
Stability-indicating method with liquid chromatography
An HPLC system (Shimadzu, Noisiel, France) was used to quantify vancomycin. It was equipped with a degassing DGU-20A3R unit, two LC-20ADXR solvent delivery units (Prominence UFLCXR series), an SIL-20ACXR autosampler, a CTO-20AC column oven and an SPD-M20A photodiode array detector (DAD).
The mobile phase, adapted from Jesús Valle et al’s method14 (8:92, v/v), was composed of acetonitrile and phosphate buffer (6.8 g/L) diluted in ultrapure water and adjusted to pH 4 with orthophosphoric acid. The flow rate was fixed at 1.2 mL/min and each run lasted 10 min. Separation of vancomycin was carried out on a Kinetex C18 column (100×4.6 mm id, 2.6 µm) preceded by a C18 cartridge guard (4.6 mm) (Phenomenex, Le Pecq, France). The injection volume was 20 µL and quantification was performed at 280 nm.
The degradation protocol complied with the SFPC/Gerpac methodological guidelines.15 To obtain about 20% degradation of vancomycin, the following conditions were used: heat (+80°C, for 300 min), acidity (+20°C, 4 N hydrochloric acid, for 2 hours), basicity (+20°C, 4 N sodium hydroxide, for 15 min) and oxidation (+20°C, 1% hydrogen peroxide, for 3 hours). The vancomycin solution was diluted to a theoretical concentration of 100 µg/mL, regardless of the degradation conditions tested. Samples were then analysed by HPLC-DAD.
To validate the HPLC-DAD method, working solutions were prepared and diluted in WFI to reach concentrations ranging from 40 to 200 µg/mL (40, 60, 80, 100, 120, 140 and 200 µg/mL). Validation was carried out on three consecutive days by determining the following parameters: specificity, linearity, limits of detection (LOD) and limits of quantification (LOQ).16 17
To assess chemical stability, vancomycin concentration was expressed as the ratio, in percentage, of the concentration measured at sampling times to the initial concentration in the syringe before infusion (Ct/C0, %). The solution was considered stable if the concentration remained ≥90% of C0. The cumulative amount over 24 hours was also calculated to appreciate the amount of vancomycin administered. The percentage loss corresponds to the following equation:
with the following theoretical amounts of vancomycin: 4 g, 3 g, 2 g or 500 mg.
Preparation of vancomycin syringes
For each studied concentration, two reconstitution solvents were used: WFI and saline solution. Vials were reconstituted either with WFI and diluted in saline solution, following SmPC recommendations, or reconstituted and diluted in saline solution, following current practice in our clinical units. The protocol is summarised in table 1.
Protocol for obtaining clinical concentrations of vancomycin
All samples were prepared and standardised by the same experienced operator, at 25°C±2°C. Vials were reversed 10 times to mix the solvent homogeneously, then were left for 1 hour to obtain complete dissolution of the lyophilisate. They were then shaken again before preparing the polypropylene syringes (20 or 50 mL) (Becton-Dickinson, Le Pont-de-Claix, France) and starting the infusion through or without an inline filter.
Infusion protocol
Vancomycin stability was tested during continuous infusion through a polyethylene infusion line (length=150 cm and internal diameter=1 mm, reference: PE1155.15; Vygon, France). Room temperature was set at 25°C±2°C. Solutions were infused by syringe pumps (Orchestra, Fresenius Kabi, Sèvres, France). Two parallel experiments were carried out. The first experiment was with inline filters in two categories: (1) with a 0.2 µm inline filter, reference NEO96E, for paediatric patients with a 25 mg/mL vancomycin solution infused at 0.8 mL/hour and (2) with a 0.2 µm inline filter, reference AEFF1NTE, for adult patients with 40–60 and 80 mg/mL vancomycin solutions infused at 2 mL/hour (Pall Corporation, Saint-Germain-en-Laye, France). The filters positioned at the end of the infusion line can sustain flow rates of up to 100 mL/hour and 540 mL/hour, respectively. The second experiment was performed under the same flow rate conditions but without an inline filter. The flow rate was constant for 24 hours to ensure total infusion of the syringe.
Visual observation was made during the infusion and sample solutions were collected at the egress of the infusion line every 2 hours. If no particle was observed, vancomycin level was measured by HPLC-DAD (n=5 syringes). All samples were diluted in saline solution to obtain a theoretical concentration of 100 µg/mL. No degradation products were found in the chromatograms obtained during the infusion protocol.
Osmolality and pH measures
Osmolality (3300 Micro-Osmometer, Advanced Instruments, Norwood, USA) and pH (SB70P Symphony, VWR International, Fontenay-sous-Bois, France) were measured for each vancomycin solution at the onset and end of infusion (n=3).
Particulate counting
Vancomycin solutions in syringes were analysed using a particle counting system (APSS-2000, Particle Measuring Systems, Dourdan, France) following Monograph 2.9.19 of the EP. For each infusion condition, three 5 mL samples from three syringes were analysed using the light obscuration counter (n=9) at time 0 (T0) and at 24 hours (T24). The number of particles ≥10 µm and ≥25 µm should not exceed 6000 and 600 particles per syringe, respectively.18
Statistical analysis
The Mann-Whitney U test compared the following filtered and unfiltered measurements: cumulative amount with both reconstitution solvents at T24, and the number of particles, pH and osmolality at T0 and T24. Statistical testing was done at the two-tailed α level of 0.05. Data were analysed using Xlstat software (Microsoft Excel, V.16.15, Addinsoft, Paris, France).
The results for pH, osmolality and number of particles were expressed as median (IQR).
Results
Stability-indicating method and HPLC-DAD validation
Under heat degradation, two degradation peaks were obtained (retention time (RT)=1.25 min and 2.80 min); under acidic and basic degradations, one peak at 5.00 min and 1.25 min, respectively, was obtained, whereas no peak was obtained in oxidative degradation conditions. All the degradation peaks presented different RTs from that of vancomycin, which was 3.08 min. No degradation products were detected on the chromatograms during the stability study.
Dosage was validated using a linear regression model. Good linearity was shown over the whole concentration range (40–200 µg/mL, r2=0.993). LOD and LOQ were 11.87 µg/mL and 23.73 µg/mL, respectively. The measured concentrations were back-calculated using the selected calibration model, and relative bias (trueness) was calculated. Relative bias was inferior to 1% over the whole calibration range (online supplementary data, table 4).
Supplemental material
Chemical stability during the 24-hour infusion
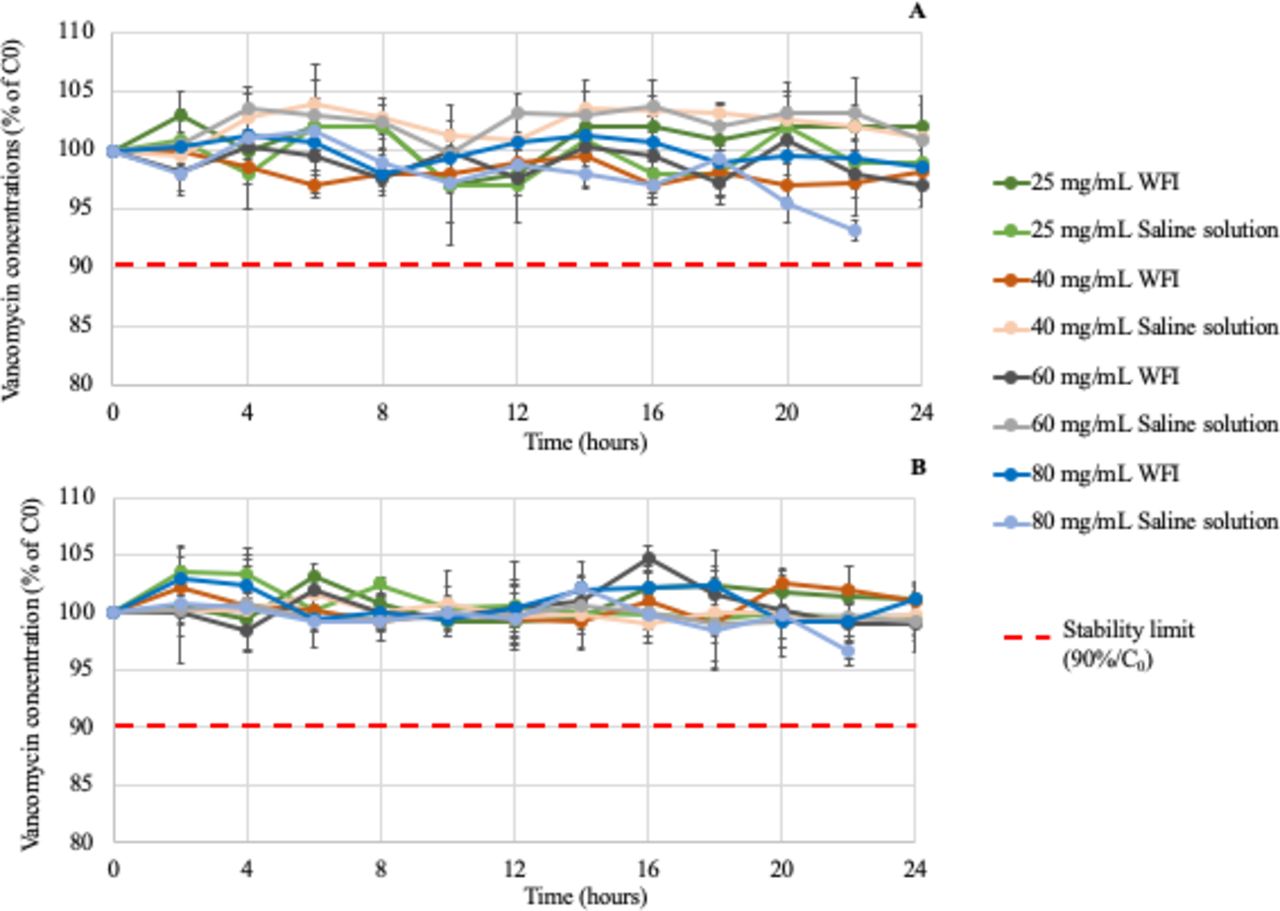
The results demonstrated stability during the 24-hour infusion: the percentage of vancomycin concentration remained over 90% (figure 1). However, for vancomycin at 80 mg/mL reconstituted and diluted in saline solution, visible particles were observed in syringes after 22 hours, so sample dosage at T24 was not carried out.
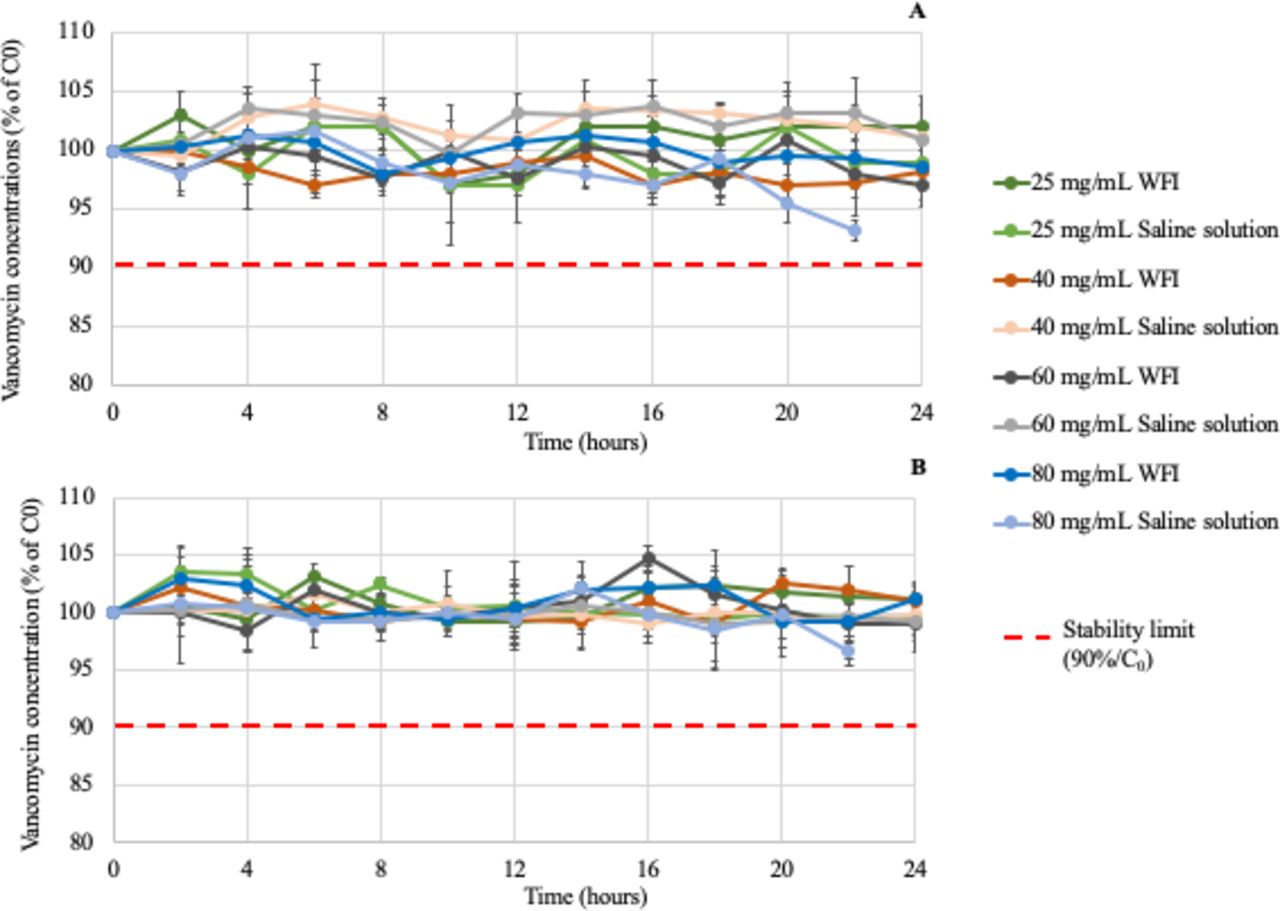
Stability profiles of vancomycin syringes during the 24-hour infusion at +25°C (A) with inline filters and (B) without inline filters (n=5). Data are presented as mean±SD. WFI, water for injection.
The cumulative amount of vancomycin in all syringes is shown in table 2.
Cumulative amount of vancomycin infused over 24 hours at 25°C (n=5 syringes), infused at 0.8 mL/hour for vancomycin syringes at 25 mg/mL and at 2 mL/hour for vancomycin syringes at 40–60 and 80 mg/mL
Osmolality and pH values
The median (IQR) osmolality was 19 (12) mOsmol/kg and 292 (1) mOsmol/kg for pure WFI and saline solution, respectively. For vancomycin reconstituted with WFI, osmolality was very low for solutions at 40–60 and 80 mg/mL (table 3); with saline solution, osmolality was closer to blood osmolality. Osmolality was stable during infusion and there was no statistical difference between filtered and non-filtered vancomycin solutions.
Evolution of osmolality for each vancomycin condition (n=3 syringes)
The median (IQR) pH of pure WFI and saline solution was 5.10 (1) and 5.61 (1), respectively. pH was stable during infusion for all vancomycin solutions and was not statistically different between filtered and non-filtered vancomycin solutions (p>0.077).
Particulate counting
The number of particles ≥10 µm for each vancomycin solution filtered or not at T0 and T24 is reported in figure 2. All solutions without an inline filter contained more than 6000 particles ≥10 µm per syringe and so were not compatible with Monograph 2.9.19 of the EP and must not be administered to patients. With inline filters, only vancomycin solutions at 25 and 40 mg/mL contained fewer than 6000 particles per syringe.
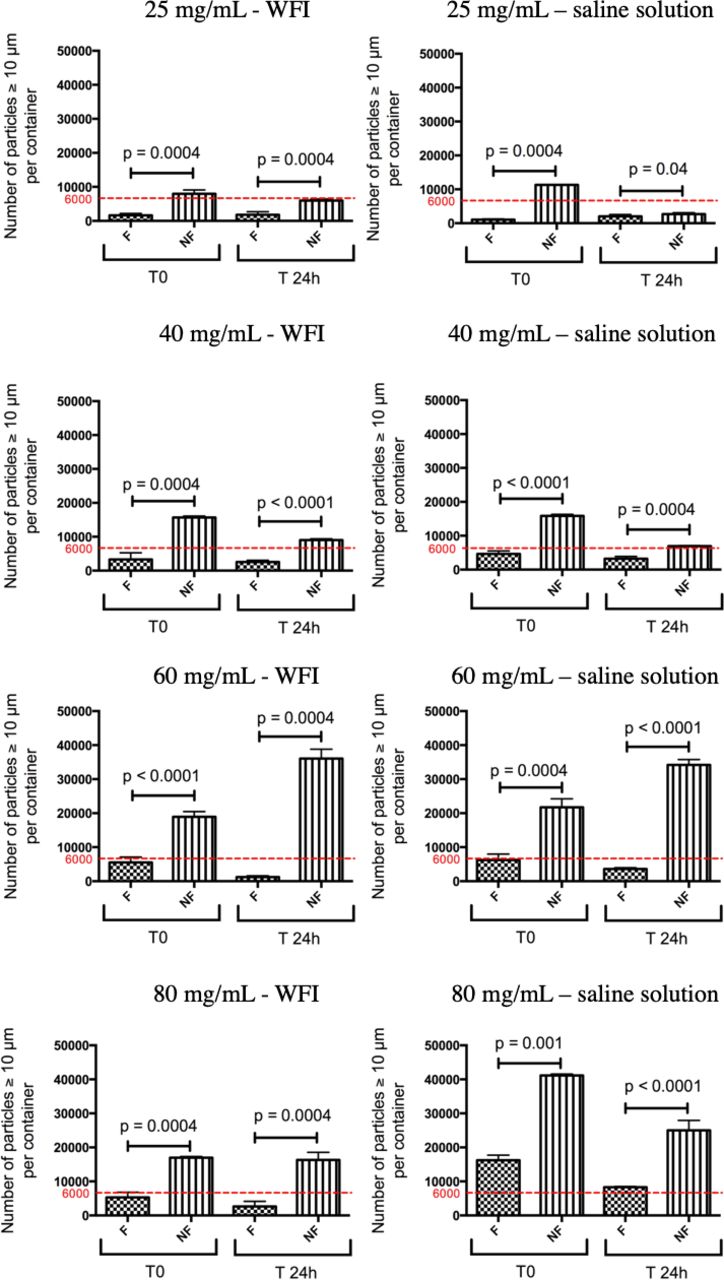
Number of particles ≥10 µm contained in vancomycin solutions (n=9). F, filtered; NF, non-filtered; T0, at time 0; T24h, at 24 hours; WFI, water for injection.
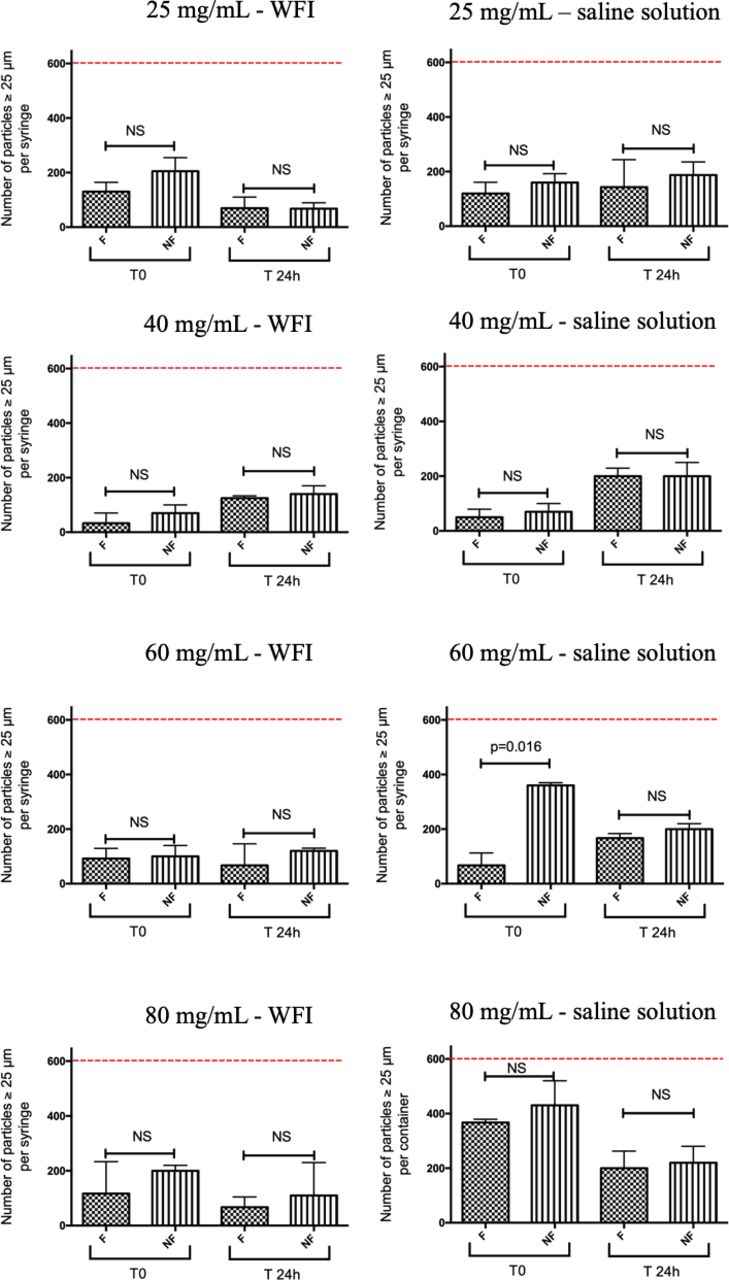
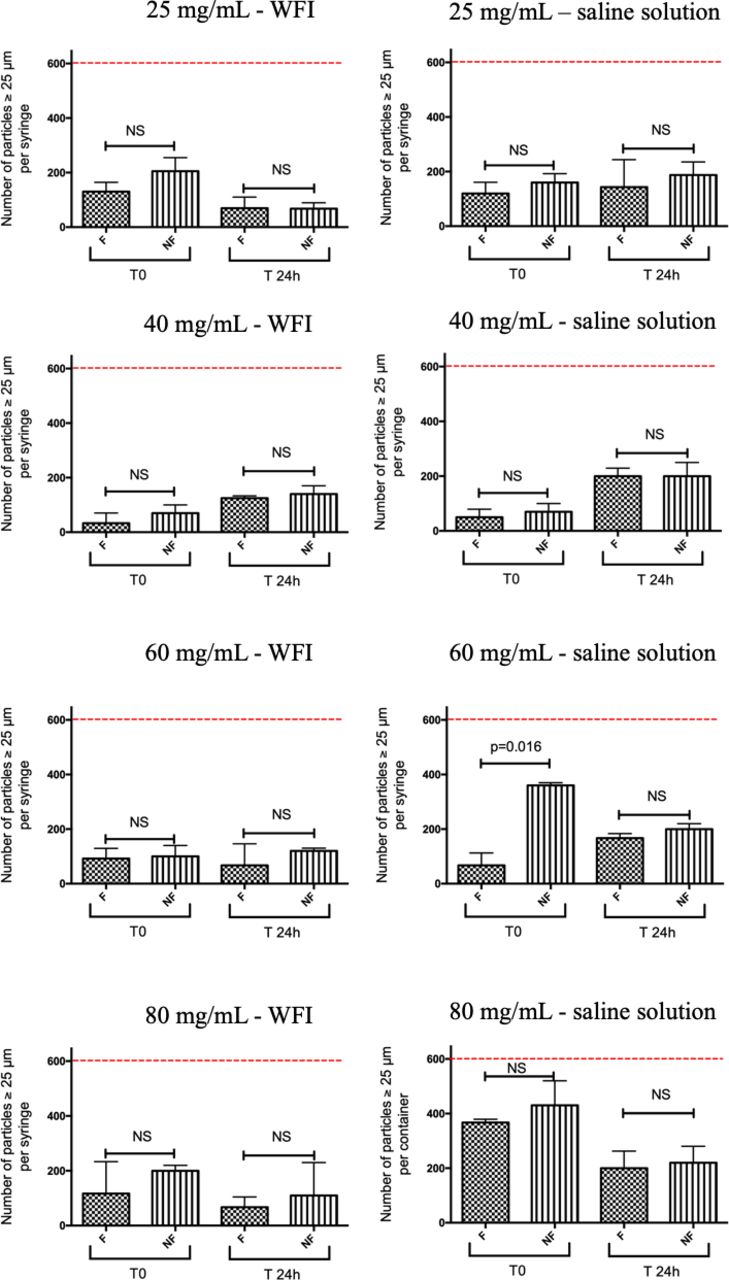
The number of particles ≥25 µm for each vancomycin solution filtered or not at T0 and T24 is reported in figure 3. All syringes contained fewer than 600 particles ≥25 µm per syringe.18 The number of particles increased according to vancomycin concentrations.
{kind=link}
{kind=link}
{kind=link}
Number of particles ≥25 µm contained in vancomycin solutions (n=9). F, filtered; NF, non-filtered; T0, at time 0; T24h, at 24 hours; WFI, water for injection.
Discussion
As previously mentioned, several studies7–10 have been conducted on physicochemical vancomycin stability but at low concentrations or in trials that do not reflect current use in care units. All published studies have been performed on solutions stocked in containers rather than in continuous infusion, with sampling at the end of the infusion line. Moreover, none has dealt with the particulate load administered to the patient. In this study, measurements of pH, osmolality, physical and chemical stability, and number of particles, with and without filter, were all carried out at different and higher concentrations compared with previously published stability studies.8 9
As for pH measurement, there was no difference at T0 and T24. Galanti et al 8 showed a significant increase in pH for vancomycin solutions at 5 and 10 mg/mL after storage at +4°C for 58 days. However, no data were provided for 24 hours at ambient temperature. Godet et al 7 found a pH of 3.17±0.01 at 41.66 mg/mL, which is close to ours at 40 mg/mL, with or without an inline filter (3.38 (1) vs 3.43 (3)). Acidic pH is not responsible for vancomycin toxicity.19 Our pH values were therefore compatible with patient administration.
The osmolality study indicated that the reconstituted solutions with WFI (as recommended in SmPC20 at 40–60 and 80 mg/mL) remained very hypotonic in 50 mL syringes, and consequently could not be injected to patients due to an osmolality inferior to 154 mOsmol/kg.21 Infusion of hypotonic solutions is associated with an increase in hyponatraemia22 and can lead to cellular necrosis. Nevertheless, for syringes with 25 mg/mL concentration, the solution remained hypotonic, although osmolality was superior to the above threshold, indicating that they should be administered with caution.
All vancomycin solutions reconstituted and diluted with saline solution were isotonic to blood (table 3). Our osmolality values were therefore compatible with patient administration, although the preparation did not follow SmPC recommendations. Hence, it is important to choose publications studying reconstitution and dilution in saline solution for vancomycin infusion by syringe.7
All vancomycin solutions were physically stable during a 24-hour infusion, except for 80 mg/mL reconstituted and diluted in saline solution. Indeed, visible particles appeared in syringes between the 22nd and 24th hour of infusion at 25°C±2°C. After 24 hours at room temperature, with high concentrations, a gel formation was observed in the syringes. This can be explained by the presence of mannitol as an excipient.
The percentage loss of a cumulative amount of vancomycin during a 24-hour infusion was statistically different for the two solvents (WFI and saline solution) at 40–60 and 80 mg/mL solutions (table 2). The cumulative amount of vancomycin was also statistically different between filtered and non-filtered 60 and 80 mg/mL solutions. However, these differences (<15%) were not clinically relevant and could be considered as equivalent. This might be due to the reconstitution of vancomycin lyophilisate in marketed products that may contain 85%–115% of the indicated quantity of active drug. However, the loss was greater for higher concentrations of vancomycin (60 and 80 mg/mL), suggesting a lyophilisate dissolution problem, as syringes were uniformly prepared. Indeed, SmPC20 recommends 20 mL for 1 g of vancomycin, which is rarely practised in care units.
For all vancomycin solutions (figures 2 and 3), the results of particulate counting showed a marked presence of subvisible particles, and for 80 mg/mL in saline solution visible particles were observed. No other published study has considered particle counting, although it seems to be essential when using an intravenous solution. Vancomycin syringes containing more than 6000 particles ≥10 µm must not be administered to patients as they can have a clinical impact: central venous catheter obstruction, potentially fatal embolism, and other forms of clinical organ failure such as systemic inflammatory response syndrome and pulmonary toxicity.23 24 The number of particles ≥25 µm was in all cases under the threshold (600 particles), regardless of the concentration considered and the solvent used.
No non-filtered vancomycin solutions, regardless of the concentrations considered, concorded with the EP with regard to particles ≥10 µm, whereas it was satisfactory for particles ≥25 µm. Although the EP refers to postproduction quality control, particle counting after 24 hours of infusion reflects the particulate load administered to the patient during infusion.
With a 0.2 µm inline filter, particulate load was minimised. Only vancomycin solutions at 25 and 40 mg/mL reconstituted in all solvents with filter, compliant with Monograph 2.9.19 of the EP,18 could be administered to patients. However, due to osmolality values, 40 mg/mL solutions reconstituted with WFI should not be administered. For 60 and 80 mg/mL solutions, the high number of particles was certainly due to precipitation occurring beyond the filter as well as solubility problems (drug and/or excipients). Particle formation could be at the origin of vancomycin toxicity as reported by Luque et al,25 who found aggregates of nanospheric vancomycin which could result in acute renal failure. Their results were confirmed by immunohistochemistry in mice and showed the impact of vancomycin particles on kidney toxicity.
With our results, some complementary studies are required to establish the precise nature and origin of particles (vancomycin, mannitol). Indeed, different specialties may produce different particulate contamination,26 which is affected by numerous parameters, such as the quality of the active substance, excipients, solvents, conditions, manufacturing processes and clinical preparation practices. An optimised protocol can reduce vancomycin dosage variations and enable homogeneous preparations.27 Indeed, variations in vancomycin dosage were due to the reconstitution solvent (saline solution) and the non-systematic practice of homogeneously mixing the lyophilisate.27
From this study, recommendations can be made for vancomycin infusion in care units. A 50 mL syringe should not contain more than 40 mg/mL of vancomycin reconstituted in saline solution and a 0.2 µm inline filter must be used for infusion. The maximum concentration in a 20 mL vancomycin syringe should be 25 mg/mL.
According to our reconstitution method, a clinical protocol can be applied to prepare vancomycin syringes with 0.2 µm inline filters, if the SmPC is not applied, for the following dosages for 24 hours:
0.5 g (25 mg/mL): one 0.5 g vancomycin vial reconstituted with 10 mL of saline solution + 10 mL of saline solution as diluent, at a flow rate of 0.8 mL/hour. One syringe of 20 mL is required for 24 hours.
2 g (40 mg/mL): two 1 g vancomycin vials reconstituted each with 20 mL of saline solution + 10 mL of saline solution as diluent, at a flow rate of 2 mL/hour. One syringe of 50 mL is required for 24 hours.
3 g (30 mg/mL): one 1 g + one 0.5 g of vancomycin vials reconstituted with 20 mL of saline solution and 10 mL of saline solution, respectively + 20 mL of saline solution as diluent, at a flow rate of 4 mL/hour over 12 hours. Two syringes of 50 mL are required for 24 hours.
4 g (40 mg/mL): two 1 g vancomycin vials reconstituted each with 20 mL of saline solution + 10 mL of saline solution as diluent, at a flow rate of 4 mL/hour over 12 hours. Two syringes of 50 mL are required for 24 hours.
6 g (40 mg/mL): two 1 g vancomycin vials reconstituted each with 20 mL of saline solution + 10 mL of saline solution as diluent, at a flow rate of 6 mL/hour over 8 hours. Three syringes of 50 mL are required for 24 hours.
What this paper adds
What is already known on this subject
Vancomycin is a broad-spectrum antibiotic widely used in hospitals, and is used at a concentration of up to 30 mg/kg and infused continuously over 24 hours.
Currently, stability studies alone do not reflect the practical conditions of vancomycin use in care services.
The intravenous infusion of drug solutions must be clear, potentially free of particles, and osmolality must be compatible with blood.
What this study adds
Current protocols have been for 0.5, 2, 4 and 6 g of vancomycin infused continuously in syringes over 24 hours.
For patients’ safety, these solutions must be infused with a 0.2 µm inline filter to limit particulate contamination.
Acknowledgments
We thank Alexandra Tavernier (MA, University of Glasgow, Professeur Agrégée, France) for English language and editing assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
EAHP Statement 3: Production and Compounding.
Twitter @MorganeMasse
Contributors Conception: MM, SG, CB, BD, PO. Formal analysis: MM, AMM, NC. Investigation: MM, AMM, NC. Methodology: MM, SG, CB, BD, PO. Supervision: SG, CB, DL, BD, PO. Writing the original draft and revision: MM, AMM, NC, SG, DL, CB, BD, PO.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.