Article Text

Abstract
Trastuzumab (Herceptin) is used in neoadjuvant, adjuvant and metastatic breast cancer. Infusion reactions are a common side effect most of which are mild and easily managed, anaphylaxis occurs rarely. The summary of product characteristics recommends observation for 6 hours after the commencement of the first administration; we wanted to evaluate this practice. We assessed first administrations of trastuzumab infusions retrospectively to determine both rate and timing of reactions. Medical and nursing notes of 94 patients who had been prescribed intravenous trastuzumab in 2012 were reviewed; 2 additional patients did not have records available. Fourteen patients received palliative, 73 adjuvant and 7 neoadjuvant trastuzumab.r. Two (2%) had a reaction to trastuzumab occurring at 70 and 80 min from infusion commencement. We did not observe a reaction in the 4.5 hours after the 90 min infusion was complete. We recommend discharge with verbal and written advice immediately after uncomplicated first administration.
- ONCOLOGY
- Breast tumours < ONCOLOGY
- Trastuzumab
- Infusion reaction
- Observation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Trastuzumab (Herceptin) is a recombinant humanised IgG1 monoclonal antibody that targets the human epidermal growth factor 2 (HER2) protein, a member of the epidermal growth factor receptor tyrosine kinase receptor family. Approximately 20% of human breast cancers overexpress HER2.1 This is assessed clinically by flourescent in situ hybridisation or immunohistochemistry gene amplification.
For breast cancer overexpressing HER2, the addition of neoadjuvant trastuzumab has been shown to increase pathological complete response (pCR) rate.2 Adjuvant trastuzumab improves progression free survival (PFS), response rate (RR)3 and overall survival (OS).4 In metastatic disease, trastuzumab with paclitaxel or monotherapy after first-line chemotherapy improves OS, PFS and RR.5 Dual anti-HER2 therapy, a combination of pertuzumab and trastuzumab plus docetaxel is now treatment of choice as first line in the metastatic setting.1 Dual anti-HER2 therapy plus docetaxel increases pCR rate and has become standard in the neoadjuvant setting in the UK as approved by National Institute for Health and Care Excellence.6 Trastuzumab is administered as an infusion or more recently as a subcutaneous injection every 3 weeks.7
Trastuzumab side effects include pulmonary and cardiac toxicity, including left ventricular dysfunction.1 Infusion-related reactions (IRR) are managed with oral medication and reported in up to 40%, with anaphylaxis in 0.25% of patients.8 Onset of mild-to-moderate symptoms such as chills, fever, hypotension and dyspnoea are classified as an IRR; these symptoms are poorly defined and so lead to a variation in IRR rates in the literature. A retrospective review of 197 patients demonstrated IRR in 16% and anaphylaxis in 1%.9 A large retrospective analysis of 25 000 patients shows anaphylaxis in 0.3% of patients.10 It is clear from the literature that IRR and anaphylaxis occur most frequently during or immediately after the first infusion.8–10
There are rare postmarketing reports of severe and fatal episodes of anaphylaxis and pulmonary toxicity. A meta-analysis included 22 randomised control trials and found that fatal adverse events for those receiving HER2 blockade (trastuzumab) were not statistically different to those in the non-HER2 blockade group.11 A PubMed search generates one case12 of severe pulmonary toxicity occurring 90 min into the first infusion, a second developing severe infusion reaction after 2 min of the first infusion13 and a third developing severe infusion reaction after 30 min of the first infusion.14
Severe infusion reactions/anaphylaxis and IRR are seldom identified during the period of observation after completing trastuzumab infusion. Thus, we hypothesise that the period of observation after the first infusion is clinically unnecessary and costly to the National Health Service. We performed this review to determine if a period of observation was necessary.
Materials and methods
Our sample consisted of 96 female patients with breast cancer who had been prescribed at least one cycle of Intravenous trastuzumab between I January 2012 and 31 December 2012, generated from in-house pharmacy software. Medical and nursing notes were retrospectively reviewed for documentation of trastuzumab reactions during the 6-hour stay from the start of the first infusion. Data were stored and processed on confidential Excel files. A retrospective approach was taken to reduce IRR reporting bias and to aid rapid data collection. From the list of 96 patients, 2 patients were excluded; in both instances, detailed records were not available.
Results
The total sample size consisted of 94 female patients with a mean age of 54 years. Fourteen patients received palliative, 73 adjuvant and 7 neoadjuvant trastuzumab. Seventeen had a documented allergy to at least one drug. Two patients had a reaction to docetaxel prior to trastuzumab; neither went on to react to trastuzumab.
Ninety two of 94 (97.9%) had no reaction to first dose of trastuzumab during the infusion or subsequent period of observation. Two had a reaction during the first infusion of trastuzumab (2.1%) and we document these here:
Case 1
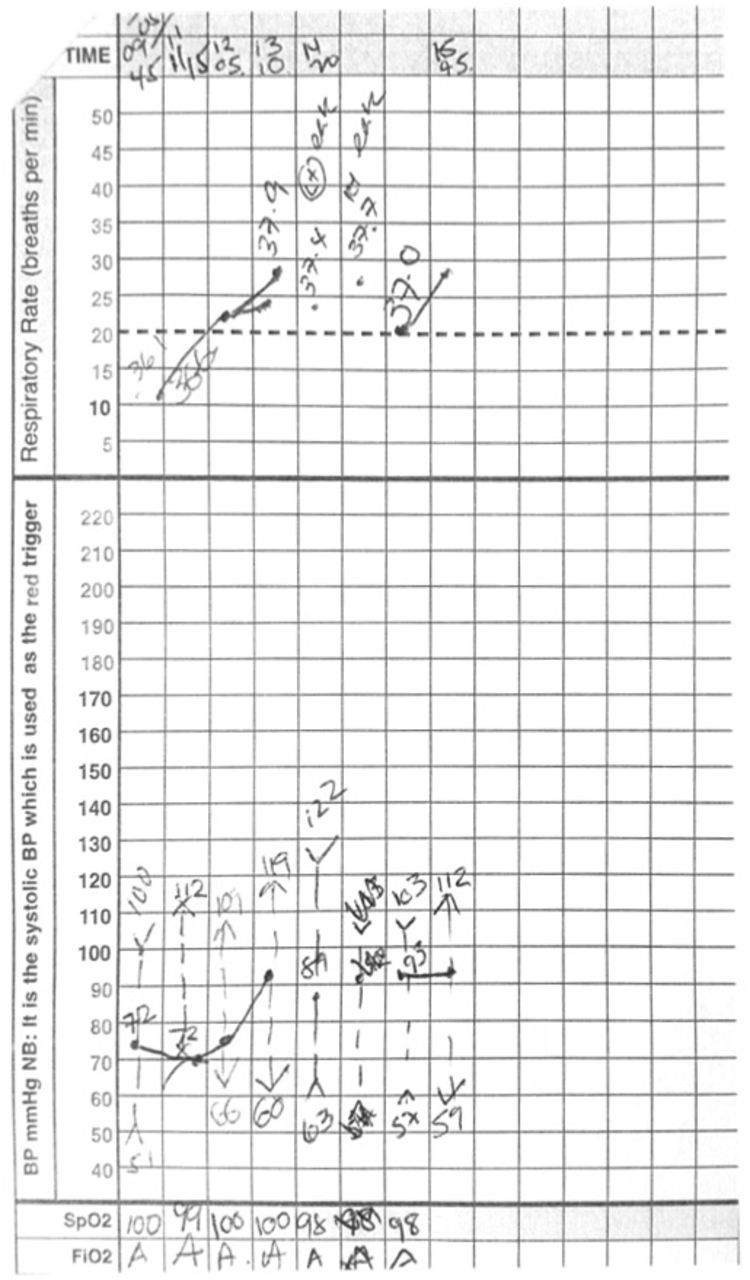
Forty four-year-old patient with right-sided grade 3, T2N0M0 ER-positive and HER2-positive ductal carcinoma of the breast treated with adjuvant E-CMF (epirubicin, cyclophosphamide, methotrexate and 5-fluorouracil) chemotherapy. She had no history of allergies, took citalopram for depression and had no other significant past medical history. Seventy minutes after commencing the first infusion, she described feeling cold and was observed to be shivering. The infusion was stopped immediately and she received 10 mg IV chlorphenamine and 100 mg IV hydrocortisone with good effect. The infusion was restarted 35 min later. She was observed for 4 hours postinfusion with no further symptoms or signs of reaction (see figure 1). She did not react to the subsequent 17 infusions of trastuzumab and received secondary prophylactic chlorphenamine and hydrocortisone.

Case 1 observation chart showing reaction to trastuzumab after 70 min.
Case 2
Seventy two-year-old lady with right-sided grade II, T1N1M0 ER-negative and HER2-positive invasive ductal carcinoma of the breast. Comorbidities included previous transient ischaemic attack and cardiac arrhythmia controlled with a pacemaker. She had not suffered a myocardial infarction and her cardiac symptoms were stable. She had documented sensitivities to indomethocin and mepore dressings. A pretreatment echocardiogram showed an ejection fraction of 64%, and thus she treated with adjuvant CMF chemotherapy.
She developed rigours after 80 min of commencing first trastuzumab infusion. The infusion was stopped and she was given 100 mg IV hydrocortisone and 10 mg IV chlorphenamine. After 55 min, the symptoms had resolved and the infusion was restarted (see figure 2). She had no further signs or symptoms after being observed for 4 hours after the infusion and went on to have subsequent infusions without reaction but with the co-administration of chlorphenamine and hydrocortisone.

{kind=link}
{kind=link}
Case 2 observation chart showing reaction to trastuzumab after 80 min.
Discussion
IRR are most likely during the first trastuzumab administration. The cause is unknown but the mechanism is unlikely to be IgE-mediated hypersensitivity as there is no prior exposure to the molecule. Trastuzumab interacts with HER2 receptors on cell membranes which leads to the release of proinflammatory cytokines. This may result in symptoms of chills, breathlessness and hypotension.2 Thus, IRR are most common at first exposure as shown clinically in a retrospective series of 197 patients (1788 doses) of which IRR occur on only three subsequent infusions.9
The risk of a subsequent reaction to an allergen within 72 hours without re-exposure to the trigger is defined as a biphasic reaction. It is the risk of biphasic reaction and delayed acute allergic reaction that explains the recommended 4 hours observation postinfusion with trastuzumab. The exact mechanism of biphasic reactions is unknown; a review of 541 case of anaphylaxis within the emergency department found that biphasic reactions were more likely with either an unknown precipitant (non-drug-related reactions) or moderate-to-severe reactions.15
We have documented reactions in only 2 of 94 (2%) patients receiving the first trastuzumab infusion, both occurring during administration. We provide evidence reactions are unlikely in the observation period postadministration of trastuzumab. A review of infusion reactions with various monoclonal antibodies concluded that reactions are likely to occur within minutes of the first infusion.16 Furthermore, a study in 2014 reports infusion reaction in 1.8% of doses of trastuzumab administered in 197 cases,9 with the majority of reactions occurring with the first dose and all reactions occurred during the infusion (between 5 and 92 min from start of infusion). As a result of a literature review and our own observations, we suggest that the practice of observation for a total of 6 hours from the start of the first infusion or subcutaneous injection of trastuzumab is unnecessary, providing the administration has been uneventful.
Seventeen of 94 patients had documented allergies and 2 of 94 had previous reactions to chemotherapy but none of these reacted to the first infusion of trastuzumab. We have seen a 2% rate of IRR, similar to recent reviews and adverse drug reactions (ARD) reporting data. We have no evidence of reaction after stopping the infusion from our 94 patients which supports the published literature.12 ,14
Adjuvant trastuzumab remains standard for this group of patients but a trastuzumab–pertuzumab combination is now licenced for first-line metastatic and neoadjuvant therapy. Large studies that led to licencing of trastuzumab and pertuzumab in both metastatic and neoadjuvant setting both report grade III/IV hypersensitivity/anaphylaxis reactions in 2% compared with 2.5% in those receiving trastuzumab alone.1 ,6 Our recommendation to abandon the period of observation postinfusion for uncomplicated cases can be extrapolated to include those treated with combination therapy.
Conclusion
IRR are common and poorly defined, serious anaphylactic reactions are rare and occur during administration of trastuzumab. We demonstrate IRR occur in 2% of patients, only during administration. We recommend discharging patients after uncomplicated first and subsequent infusions or subcutaneous injections of trastuzumab with verbal and written advice without an additional period of observation.
References
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.