Article Text

Abstract
Background and objective Infusion containing paracetamol, alizapride, ketorolac and tramadol is used after a general anaesthesia in order to limit pain, fever and nausea. Currently, these infusions are prepared according to demand in the anaesthesia unit, but the preparation in advance could improve quality of preparation and time management. The aim of this study was to investigate the long-term stability of this infusion in glass bottles at 5°C ± 3 °C.
Method Five bottles of infusion were stored at 5°C ± 3 °C for 60 days. A visual and microscope inspection were performed periodically to observe any particle appearance or colour change. pH and absorbance at three wavelengths were measured. The concentrations were measured by ultra-high performance liquid chromatography – diode array detection.
Results Multiple verifications were performed during the first 35 days and no crystal, impurity or colour change were observed. At the next time point (42nd day), crystals were visible to the naked eye. pH and absorbance at 350 nm and 550 nm were stable. A slight increase in the absorbance at 410 nm was observed during the study, suggesting that a degradation product could be formed and absorb at this wavelength. The infusion was considered chemically stable while the lower one-sided prediction limit at 95% remains superior to 90% of the initial concentration. Concentration measurements demonstrated that ketorolac and alizapride remained stable in the infusion for 35 days. The stability of tramadol was 28 days. However, degradation of paracetamol was much faster given that concentration has fallen below 90% of the initial concentration after 7 days.
Conclusion Infusion of paracetamol, alizapride, ketorolac and tramadol remains stable for 7 days in glass bottles at 5°C ± 3 °C and could be prepared in advance with these storage conditions.
- paracetamol
- alizapride
- ketorolac
- tramadol
- UHPLC
- drug stability
Statistics from Altmetric.com
Introduction
During the post-operative period, multimodal analgesia is recommended to manage patient pain efficiently. The multimodal strategy consists in injecting several drugs with different analgesic mechanisms to benefit from the synergy of their actions and minimise side effects by using optimal dosages for each agent.1–5 In order to limit the number of injections, it is common for anaesthesia staff to mix all the components of infusion and inject patients only once. Therefore, patients are perfused with a combination of paracetamol, alizapride, ketorolac and tramadol to limit pain, fever, nausea and vomiting after a general anaesthesia.
Paracetamol is an analgesic and antipyretic drug widely used because of its good tolerance and its weak adverse effects.6 7 Tramadol acts as a weak opioid agonist and relieves mild to severe post-operative pain. However, it can cause adverse events, such as nausea and vomiting.3 8 Ketorolac is also an analgesic and is a part of the nonsteroidal anti-inflammatory drugs (NSAIDs) family. It is used in combination with opioid to achieve an adequate analgesia while limiting side effects.9 In addition to pain, nausea and vomiting are common inconveniences after surgery under general anaesthesia.10 Post-operative nausea and vomiting can be prevented by alizapride, an antiemetic agent.10 11
Currently, infusions containing the four active principles are reconstituted according to demand by the anaesthesia staff. However, these infusions could be prepared in advance by a Centralised Intravenous Additive Service (CIVAS) to improve time management and preparations quality.12 13 This purpose requires the awareness of the stability of each component in the infusion. Some data are available about the compatibility and stability of alizapride with tramadol,14 ketorolac with tramadol,15 16 paracetamol with tramadol17 and paracetamol with ketorolac.18 Nevertheless, long-term stability of the quaterny mixture remains unknown. At anaesthesia unit request, the stability of infusion containing paracetamol, alizapride, ketorolac and tramadol was assessed in glass bottle at 5°C±3°C in order to evaluate the possibility of a centralised preparation. Consequently, the anaesthesia unit could be provided with ready-to-use injectables containing the four drugs.
Materials and methods
Solutions preparation
Five bottles of infusion were prepared under aseptic conditions by injection of alizapride (Litican 50 mg/2 mL, lot DY007, Sanofi, Diegem, Belgium), ketorolac (Taradyl 10 mg/1 mL, lot F1015F01, Atnahs, London, United Kingdom) and tramadol (Contramal 100 mg/2 mL, lot 009231, Grünenthal, Nanterre, France) in glass bottles of paracetamol (1 g/100 mL, lot 14LI38, Fresenius Kabi, Schelle, Belgium). Final solutions contained approximately 476 µg/mL alizapride, 190 µg/mL ketorolac, 952 µg/mL tramadol and 9524 µg/mL paracetamol.
Solutions were stored at 5°C±3°C during the study and aliquots were taken with following frequency: first week every day, three times per week during the second to fourth weeks' period and finally once a week during the second month. One aliquot was immediately analysed in order to assess the solutions physical stability while another one was frozen at −80°C. All samples were defrosted at room temperature at the end of the study for chemical stability evaluation.
Physical stability
Each time point of analysis, solutions were visually inspected in front of black and white backgrounds in order to observe any particle appearance or colour change. Crystals were searched under a microscope 80X (Jenamed, Carl Zeiss, Germany) after the solutions centrifugation at 2150 g for 5 min (Heraeus multifuge 1S, Thermo Scientific, USA). The stability of pH was assessed thanks to measurements with a glass electrode pH meter (InoLab, WTW GmbH, Germany). Optical densities at three wavelengths (350, 410 and 550 nm) were measured with a spectrophotometer (Genesys 10 UV, Spectronic Unican, USA) to test turbidity and detect subvisible particles.19
Chemical stability
Chromatographic conditions
Molecules concentrations were measured by chromatography. Analyses were performed with an ultra-high performance liquid chromatography (UHPLC) system coupled with photodiode array (PDA) detection (Acquity, Waters, Milford, USA) and Empower 3 as processing software (Waters). A reverse phase column (Acquity UPLC BEH C18 130 Å 1.7 µm 2.1 mm X 100 mm, lot 0311380032, Waters) with a pre-column (Acquity UPLC BEH C18 VanGuard Pre-column 130 Å 1.7 µm 2.1 mm X 5 mm, lot 0307372572, Waters) was used at 30°C with a flow rate of 0.6 mL/min. A gradient separation was carried out with water pH 2 (adjusted with phosphoric acid 85 wt. % in water, Sigma-Aldrich, lot MKCB7708, Saint-Louis, USA) and acetonitrile (Biosolve, lot 1215101, Dieuze, France). The run started with a low organic content (10%) for 2 min before being gradually increased to 45% in 4 min. Conditions were kept during 1 min and the column was then reequilibrated for 3 min. 5 µl of 1:100 diluted samples in water (B. Braun, lot 180218091, Melsungen, Germany) were injected. Chromatograms were extracted from wavelengths scan at absorption maximum for each molecule: 243 nm (paracetamol), 223 nm (alizapride), 312 nm (ketorolac) and 215 nm (tramadol).
UHPLC was also coupled with a QDa detector (Acquity, Waters) for full scan mass analyses. The same conditions were used except the aqueous phase for the elution gradient which was 0.1% formic acid (Biosolve, lot 1198871, Dieuze, France) in water.
Standard and control solutions
Standard and control solutions were prepared each working day by dilution of a fresh mixture of paracetamol, alizapride, ketorolac and tramadol in purified water in the same proportion as the studied infusion. A calibration curve was carried out based on five levels of calibrator and a weighted regression procedure (1/X) was performed. Three levels of control were used (table 1). Solutions were diluted 1:100 in water before UHPLC injection.
Calibrators and controls concentrations
Validation of the UHPLC method
Following the ICH Q2 (R1) guidelines, the chromatographic method was validated based on linearity, precision, detection and quantification limits. A forced degradation study was also carried out to assess the stability-indicating capability of the method.20
Linearity
The range of linearity was determined once by two-fold serial dilutions (14 dilutions were performed) from a fresh mixture containing 13 334 µg/mL paracetamol, 668 µg/mL alizapride, 267 µg/mL ketorolac and 1333 µg/mL tramadol. A highly concentrated mixture was used in order to verify that injectables could be quantified in the linearity range. All solutions were diluted 1:100 in water before injection.
Precision
Precision was considered at two levels: repeatability (intra-day) and intermediate precision (inter-day). Both levels were evaluated by 10 measurements for three concentrations, corresponding to controls used every working day.
Detection and quantification limits
Limits of detection (LOD) and quantification (LOQ) were calculated based on mean and SD obtained for water injections (n=10). LOD was estimated as mean plus three times the SD and LOQ as mean plus 10 times the SD.
Stability indication
Six conditions were tested for forced degradation of solutions containing only one active principle (paracetamol, alizapride, ketorolac or tramadol): natural, acidic (HCl) and basic (NaOH) conditions before and after heating at 100°C for 1 hour. Samples were injected in UHPLC and interfering peaks were searched in each chromatogram extracted at the specific wavelength of the studied molecule.
Chemical stability study
Aliquots of a same bottle of infusion were defrosted at room temperature for UHPLC analysis the same day. This allowed a reduction in results variability within a same bottle due to experiment conditions. Samples were diluted 1:100 in triplicate in purified water before injection.
Statistical analysis
As defined in the ICH Q1E, the shelf life of the product was defined as “the earliest time at which the 95 per cent confidence limit for the mean intersects the proposed acceptance criterion”.21 Therefore, a unilateral 95% CI on the mean was used to determine the earliest time at which the product concentration fall under 90% of the initial concentration or 95% of the initial concentration when any signs of physical instability exist.22
However, as stated by the Shelf-Life Working Group of the Product Quality Research Institute, the definition of the shelf life should be based on “an acceptably small proportion of product exceeding an acceptance criterion”.23 We thus confirmed our analyses with the use of 95% unilateral prediction interval in lieu of the CI. A 95% prediction interval is an interval that covers, on average, 95% of the distribution.
Results and discussion
Physical stability
No crystal, impurity or colour change were observed during the first 35 days of storage at 5°C±3°C. At the next time point (42nd day), crystals were visible to the naked eye in all bottles. The physical stability study was, therefore, stopped after 42 days. In order to assess the temperature effect, bottles were kept at room temperature and dissolution of crystals was visible after 3 days. pH (mean±SD: 5.88±0.06) and absorbance at 350 nm (2.377±0.095) and 550 nm (0.000±0.001) were stable during the study, including while crystals appeared. Despite a low absorption at 410 nm, a slight increase in the absorbance at this wavelength (0.004±0.003) was observed during the 42 days, suggesting that a degradation product could be formed and absorb at this wavelength.
UHPLC method development
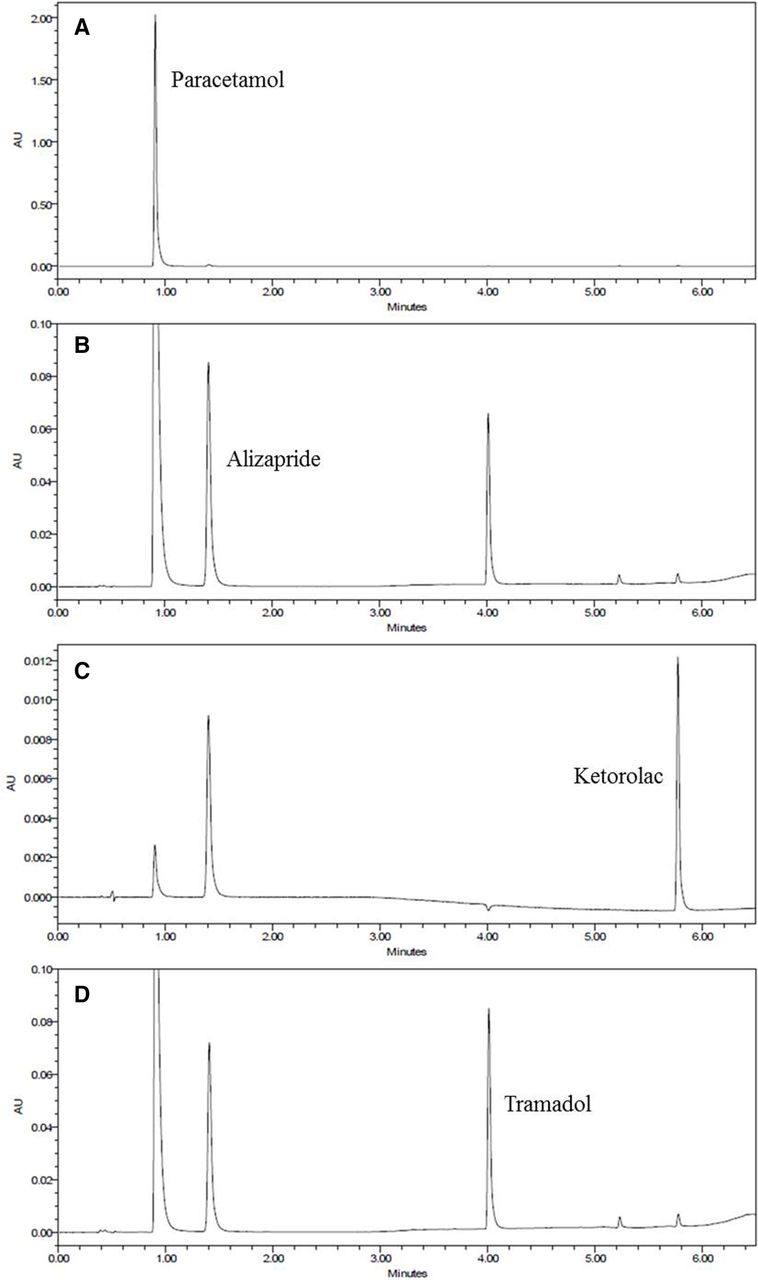
Molecules chemical structures were examined before starting the method development. The logarithm of the partition coefficient (Log P) for each component indicated that molecules were hydrophobic (paracetamol: 0.91, alizapride: 1.13, ketorolac: 2.28, tramadol: 2.45), suggesting the use of a C18 column. pH-distributions of species were analysed to determine pH of the mobile phase. It was set at pH 2, given that a unique species for each molecule was in solution at this pH, avoiding separation variability due to pH variations. Water adjusted to pH 2 with phosphoric acid (pK1 2.12) was chosen because phosphate could act as a buffer at pH of interest. A gradient elution with acetonitrile was performed to optimise separation of early eluted peaks and accelerate late elutions. The four wavelengths of analysis were chosen thanks to molecules spectra obtained with the PDA scan: wavelengths corresponding to absorption maxima were selected. Anyway, all molecules were visible on each chromatogram extracted at the chosen wavelengths, but at different intensities. Several injection volumes and sample dilutions were investigated and were fixed at 5 µl of 1:100 diluted sample in order to obtain reproducible signals without any detector saturation. Three flow rates were tested (0.4–0.5 – 0.6 mL/min) before choosing 0.6 mL/min, allowing a fast analysis and a decrease of peaks tailing. The final method allowed quantification of each molecule of interest in the studied mixture with just one UHPLC injection (figure 1).

Chromatograms obtained for injection of 5 µl of 1:100 diluted infusion (initially containing 9524 µg/mL paracetamol, 476 µg/mL alizapride, 190 µg/mL ketorolac and 952 µg/mL tramadol) at 243 nm (A), 223 nm (B), 312 nm (C) and 215 nm (D).
UHPLC method validation
Linearity, detection and quantification limits of the method (table 2) allowed correct molecules quantification in the studied injectable solution. Precision for intra- and inter-assay for quantification of each molecule was evaluated by the relative standard deviation which was lower than 2.20% (table 3). A forced degradation test showed diminution of all peaks of interest and the appearance of some small peaks corresponding to degradation products (figure 2), especially for tramadol at acidic pH after heating (figure 2D). However, no interference with peaks of interest was detected. The UHPLC method was, therefore, stability-indicating for the four components.
Linearity, detection and quantification limits for each molecule
Precision for intra- and inter-assay for each molecule (n=10)

Forced degradation chromatograms of paracetamol (A), alizapride (B), ketorolac (C) and tramadol (D). Before heating: – natural, – acidic, – basic pH. After heating: -- natural, -- acidic, -- basic pH.
Chemical stability
Alizapride and ketorolac were stable in the infusion during the 35 first days of analysis (figure 3B,C) given that during this period the lower limit of the one-sided 95% prediction interval remained superior to 90% of the initial concentration for these molecules. Tramadol was stable for 28 days (figure 3D). However, paracetamol was stable for only 7 days (figure 3A) but no degradation product was observed on chromatograms. Given that paracetamol showed chemical instability, solutions were additionally analysed with a mass detector looking for known degradation products of paracetamol: 4-aminophenol, the main degradation product which can be formed by hydrolysis during the storage of paracetamol preparation, 1,4-benzoquinone, 4-nitrophenol, hydroquinone and N-acetyl-p-benzoquinone imine.24–28 None of them could be distinguished from the background noise. The physicochemical results allow us to add this solution to the list of our systematic studies of the long-term stability of ready-to-use intravenous drug solutions29 and the advance preparation by a CIVAS may be considered.12 13 Physicochemical stability was only evaluated and the microbiological aspects were not investigated. However, according to Chapter 797 of the United States Pharmacopoeia, this preparation can be assimilated to low-risk compounding.30

{kind=link}
{kind=link}
{kind=link}
Relative concentration evolution vs time for paracetamol (A), alizapride (B), ketorolac (C) and tramadol (D) contained in infusion bottles at 5°C±3°C. Grey dots: observations for each studied bottle, black dots: observations means, black line: mean estimated by the linear regression, grey dotted line: lower limit of the one-sided 95% CI, black dotted line: lower limit of the one-sided 95% prediction interval.
Conclusion
The stability of infusion containing paracetamol, alizapride, ketorolac and tramadol in glass bottles at 5°C±3°C was evaluated in order to prepare it in advance and provide the anaesthesia unit with ready-to-use injectables. Actually, patients are injected with this infusion after a general anaesthesia to limit pain, fever, nausea and vomiting. This study showed that the infusion was physically stable for 35 days before precipitating. However, it was chemically stable for only 7 days due to a rapid decrease of paracetamol concentration. The infusion could be prepared in advance by a centralised unit and be stored for 7 days maximum at 5°C±3°C.
What this paper adds
What is already known on this subject
Compatibility and stability of some components of the infusion were known: alone or with one another
Long-term stability of the four components (paracetamol, alizapride, ketorolac and tramadol) together in glass bottles at 5°C±3°C remained unknown
What this study adds
The infusion is physically stable for 35 days before precipitating
The four active principles are chemically stable in the infusion during 7 days
The infusion preparation in advance by a centralised unit could be considered
References
Footnotes
EAHP Statement 3: Production and Compounding.
Contributors M-LC, J-D H, LS, OC, NG and LG designed the study; M-LC and OC performed experiments; M-LC, OC and BB analysed data; M-LC and LG wrote the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.