Article Text

Abstract
Objectives Opioid-free anaesthesia is a treatment strategy of pain management based on the use of drugs such as lidocaine, ketamine and dexmedetomidine that do not interact significantly with opioid receptors. In particular, these drugs are used by anaesthesiologists to ensure adequate levels of analgesia during surgical procedures for burn patients such as daily wound dressings and graft surgeries. Furthermore, for hypothermia prevention and wound-healing purposes, ambient temperature must be kept high for these patients, usually between 27°C and 30°C. To facilitate the use of this technique, clinicians want to mix lidocaine and ketamine in the same syringe. No stability data is available to determine the feasibility of this admixture and at this temperature. The objective was to study the physicochemical stability of lidocaine 20 mg/mL with ketamine 2.5 mg/mL diluted with 0.9% sodium chloride (0.9% NaCl) stored at 28°C in polypropylene syringe for 48 hours.
Methods Physical stability was evaluated by visual examination and by measuring turbidity with a spectrophotometer. Chemical stability was determined after preparation and after 6, 24 and 48 hours of conservation with a high performance liquid chromatography and pH measurements. The method was validated according to International Conference on Harmonisation Q2(R1) guidelines.
Results Both lidocaine (99.98%±1.44%) and ketamine (100.70%±0.95%) retained more than 95% of their initial concentration after 48 hours storage. pH measurements remained stable over the course of the study (less than 0.21 point of variation). No signs of physical instability were observed after visual and subvisual inspections.
Conclusions The physicochemical stability of lidocaine 20 mg/mL and ketamine 2.5 mg/mL diluted with 0.9% NaCl in a polypropylene syringe stored at 28°C protected from light was demonstrated for 48 hours. This infusion technique is therefore feasible from a pharmaceutical point of view in burn-unit settings.
- lidocaine
- ketamine
- opioid-free
- drug stability
- anaesthesia
Statistics from Altmetric.com
Introduction
General anaesthesia consists in the balanced association of hypnotics, either intravenous or volatile, analgesics, mostly opioids, and neuromuscular blockers if indicated. Pain management is a major issue in the critically-ill burn patient. Moderate and severe pains are mainly relieved with the use of opioid medicines such as tramadol, morphine or oxycodone. Economic and highly effective, opioid medicines are widely prescribed for patients during the perioperative period, for chronic pain or cancer pain. However, these medications can cause constipation, nausea and vomiting, respiratory depression, hyperalgesia, drug tolerance and addiction. The last two side-effects cited lead some patients to substance misuse, which is the first step towards aberrant drug-related behaviour and thus these side-effects are the main disadvantage of opioid medications. Opioid addiction has become a major health concern in the United States, and is carefully monitored in France to avoid a similar crisis.1 2 In view of these considerations, prescribing other methods of pain management, whenever possible, can contribute to reduce use of opioid medicines.3
Opioid-free anaesthesia is based on the use of drugs that do not interact significantly with opioid receptors µ, κ and δ. N‐methyl‐D‐aspartate antagonists such as ketamine or magnesium, α−2 agonists such as clonidine or dexmedetomidine, acetaminophen, nonsteroidial anti-inflammatory and local anaesthetics such as lidocaine are the major medicines used.3 4 During anaesthesia, opioids can be fully replaced by these drugs. In the burn patients, for quick procedures such as daily-wound dressings, these drugs are given separately and by IV boluses. For longer procedures such as excision graft surgeries, they are given by continuous IV infusion, sometimes mixed in the same syringe, and extended for hours in the postoperative period. Furthermore, for hypothermia prevention and wound-healing purposes, ambient temperature must be kept high, usually between 27°C and 30°C.5 Stability data of lidocaine mixed with ketamine is necessary in this particular situation.
Ketamine and lidocaine are both very stable drugs in solution. Stucki MC et al demonstrated 365-day stability for 1 mg/mL ketamine, stored at 40°C in 0.9% sodium chloride (0.9% NaCl) in polypropylene syringes.6 Huvelle S et al established 180-day stability for 50 mg/mL ketamine in polypropylene syringes at 25°C protected from light.7 For lidocaine, Storms ML et al defined 90-day stability at 25°C and 20 mg/mL in polypropylene syringes and Smith FM et al described 120-day stability in glucose 5% in PVC infusion bags at 4 mg/mL at 30°C.8 9 However, no stability data of lidocaine mixed with ketamine was available.
The objective of this work was to study the stability of lidocaine hydrochloride at 20 mg/mL mixed with ketamine hydrochloride at 2.5 mg/mL diluted with 0.9% NaCl in polypropylene syringes stored at 28°C protected from light for 48 hours.
Material and method
Chemicals and reagents
Potassium dihydrogenphosphate (KH2PO4, Emsure batch AM0973577 618), sodium hydroxide 30% (NaOH, VWR chemicals batch 15K250513) and acetonitrile for HPLC isocratic grade (Carlo erba Reagents batch D8E017238) were used for the mobile phase. Hydrochloric acid 30% (HCl, VWR chemicals batch 1804003), sodium hydroxide 1M (VWR chemicals batch 17110003), hydrochloric acid 1M (batch 1804003) and hydrogen peroxide 30% (H2O2, Emsure batch K48743810 713) were used. Water for chromatography was obtained from a reverse osmosis system (Millipore Iberica, Madrid, Spain). Lidocaine 50 mg/mL solution for injection (Aspen batch: 9945375), ketamine 50 mg/mL solution for injection (Renaudin batch: 205544) and 0.9% NaCl 500 mL glass vials (C.D.M Lavoisier batches: 8F461, 8F499 and 8F495) were used for test solutions, forced degradation and the validation of the analytical method.
Preparation of test solutions
For the preparation, 2.5 mL of ketamine 50 mg/mL and 20 mL of lidocaine 50 mg/mL were diluted with 0.9% NaCl to obtain a final volume of 50 mL. These solutions were stored in polypropylene syringes (BD Plastipak, 50 mL Luer-lock). Three syringes were prepared and were stored at 28°C, protected from light.
HPLC assay
Lidocaine and ketamine solutions were analysed by a stability-indicating reversed-phase high-performance liquid chromatography (RP-HPLC) method with photodiode array detection, adapted from the European Pharmacopoeia (Eur Ph).10
The HPLC system consisted of an ELITE LaChrom VWR/Hitachi plus autosampler, a VWR photodiode array (PDA) detector L-2455 and a VWR L-2130 HPLC-pump. Data was acquired and integrated by using EZChrom Elite (VWR, Agilent). The column used was LiChrospher 100 RP-18, LiChroCART 125–4, length 12.5 cm and particle size 5 µm (Analytical Chromatography, Merck). The mobile phase was 60% of a phosphate buffer KH2PO4 at 4.85 g/L, adjusted at pH=8.0% and 40% of acetonitrile isocratic grade.
The flow rate was set at 1 mL/minute, with an injection volume of 20 µL. The detection wavelength was set at 230 nm. The temperature of the injector was set at 30°C and the temperature of the column at 40°C.
Lidocaine assay
The calibration curve was constructed from plots of peak area vs concentration. The linearity of the method was evaluated for five concentrations (120, 160, 200, 240, 280 µg/mL). The intra-day reproducibility was evaluated as recommended by International Conference on Harmonisation (ICH) Q2 (R1), using three determinations at 60%, 100% and 140% of the test concentration (ie, 120 µg/mL, 200 µg/mL and 280 µg/mL).11 Interday precision was evaluated by repeating the three determinations at the three concentrations previously mentioned for 3 days.12
The stability-indicating capability was evaluated by analysing forced degraded lidocaine solutions.
Acidic conditions: a solution of 800 µg/mL lidocaine hydrochloride 1 mL was diluted with 1 mL HCl 30% and heated at 85°C for 48 hours, neutralised by 1 mL of NaOH 30% and diluted with 1 mL of ultrapure water to obtain a theoretical concentration of 200 µg/mL.
Alkali degradation: a solution of 800 µg/mL lidocaine hydrochloride 1 mL was diluted with 1 mL NaOH 1M and heated at 85°C for 48 hours, neutralised by 1 mL of HCl 1M and diluted with 1 mL of ultrapure water to obtain a theoretical concentration of 200 µg/mL.
Oxidative degradation: a solution of 800 µg/mL lidocaine hydrochloride 1 mL was diluted with H2O2 3% 1 mL stored at ambient temperature for 48 hours and diluted with 2 mL of ultrapure water to obtain a theoretical concentration of 200 µg/mL.
UV degradation: a solution of 200 µg/mL lidocaine hydrochloride was exposed for 24 hours under a sun-like spectrum lamp at 254 nm (Vilbert Lourmat).
Heat degradation: a solution of 200 µg/mL lidocaine hydrochloride was exposed to a temperature of 85°C for 48 hours.
Ketamine assay
The calibration curve was constructed from plots of peak area vs concentration. The linearity of the method was evaluated for five concentrations (150, 200, 250, 300, 350 µg/mL). The intra-day reproducibility was evaluated as recommended by ICH Q2 (R1), using three determinations at 60%, 100% and 140% of the test concentration (ie, 150 µg/mL, 250 µg/mL and 350 µg/mL). Interday precision was evaluated by repeating the three determinations at the three concentrations previously mentioned for 3 days.
The stability-indicating capability was evaluated by analysing forced degraded ketamine solutions.
Acidic conditions: a solution of 1000 µg/mL ketamine hydrochloride 1 mL was diluted with 1 mL HCl 30% and heated at 85°C for 48 hours, neutralised by 1 mL of NaOH 30% and diluted with 1 mL of ultrapure water to obtain a theoretical concentration of 250 µg/mL.
Alkali degradation: a solution of 1000 µg/mL ketamine hydrochloride 1 mL was diluted with 1 mL NaOH 1M and heated at 85°C for 48 hours, neutralised by 1 mL of HCl 1M and diluted with 1 mL of ultrapure water to obtain a theoretical concentration of 250 µg/mL.
Oxidative degradation: a solution of 1000 µg/mL ketamine hydrochloride 1 mL was diluted with H2O2 3% 1 mL stored at ambient temperature for 48 hours and diluted with 2 mL of ultrapure water to obtain a theoretical concentration of 250 µg/mL.
UV degradation: a solution of 250 µg/mL ketamine hydrochloride was exposed for 3 hours under a sun-like spectrum lamp at 254 nm (Vilbert Lourmat).
Heat degradation: a solution of 250 µg/mL ketamine hydrochloride was exposed to a temperature of 85°C for 48 hours.
Sample dilution for analysis by RP-HPLC
The solutions were diluted before analysis with 0.9% sodium chloride to obtain the concentration of the middle of the standard curve (200 µg/mL for lidocaine and 250 µg/mL for ketamine).
The diluted solutions were analysed after preparation and after 6, 24 and 48 hours. After dilution, the samples were analysed by RP-HPLC.
Total run time was set at 28 min. A single sample was taken from each syringe each time of the assay.
Chemical stability was defined as not less than 95% of the initial concentration for both drugs.
pH measurement
pH measurement was performed using a Bioblock Scientific pH meter. Analysis was carried out for each syringe after preparation and after 6, 24 and 48 hours. pH values were considered to be acceptable if they did not vary by more than 1 pH unit from the initial measurement.
Determination of physical stability
Physical stability was realised with a visual examination: colour changes and particulate matter every day of the assay. The subvisual aspect was assessed by using a Safas Monaco UV mc2 spectrophotometer. The assay was carried after preparation and after 6, 24 and 48 hours. The absorbance light was scanned at 550 nm. The absorbance of more than 0.010 AU was considered as an evidence of turbidity, providing a quantitative determination of incompatibility. An absorbance reading less than 0.010 AU was considered to be a noise level.
Results
Reversed phase HPLC
Lidocaine assay
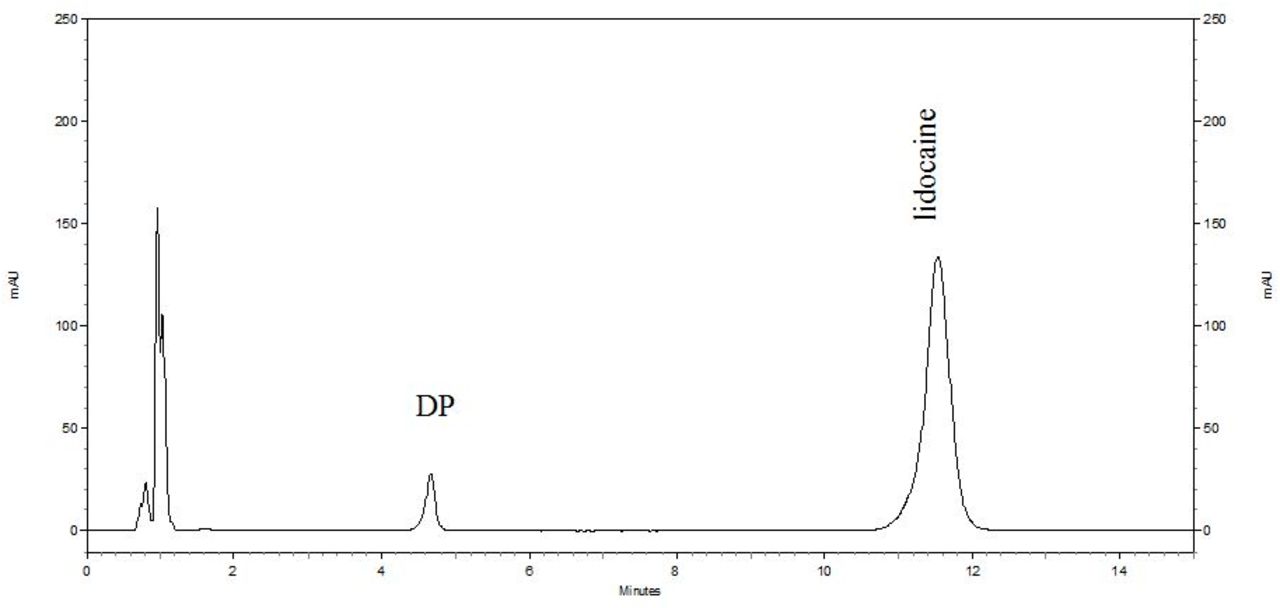
Under these conditions, the retention time of lidocaine was around 11.5 min. The calibration curve was linear, the correlation coefficient was 0.9998. The equation of the calibration curve was y=72 950.14750 x – 216 014.367. The intra-day precision expressed as relative standard deviation (RSD) ranged between 0.60% and 2.70%. The inter-day precision expressed as RSD ranged between 1.25% and 1.57%.
Stability-indicating capacity was proved by using various stressed conditions. A chromatogram obtained after acidic stressed conditions is presented in figure 1.
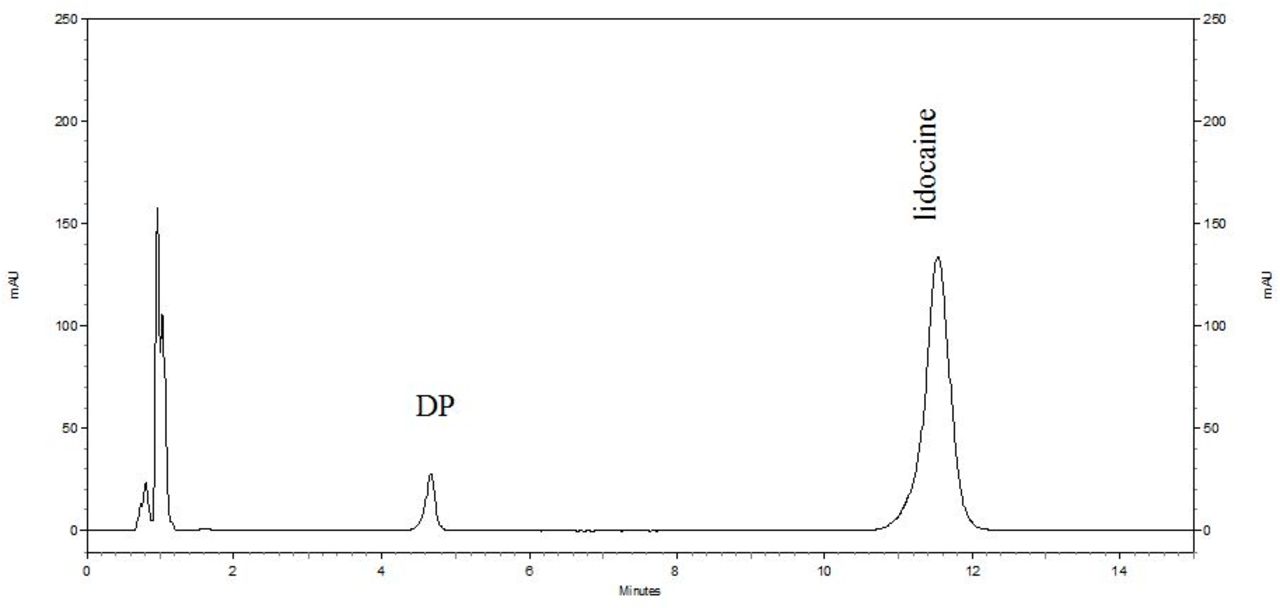
Chromatogram of 200 µg/mL lidocaine in ultrapure water after acidic stressed conditions.
The mass balance was evaluated and is presented in table 1. Area for exclusion limit was established at 5500.
Mass balance of lidocaine solutions after various stressed degradations
Ketamine assay
Under these conditions, the retention time of ketamine was around 8.2 min. The calibration curve was linear, the correlation coefficient was 0.9997. The equation of the calibration curve was y=56 588.36267 x – 94 498.733. The intra-day precision expressed as RSD ranged between 0.27% and 1.97%. The inter-day precision expressed as RSD ranged between 0.96% and 1.42%.
Stability-indicating capacity was proved by using various stressed conditions. A chromatogram obtained after photolytic stressed conditions is presented in figure 2.

{kind=link}
{kind=link}
Chromatogram of 250 µg/mL ketamine in ultrapure water after photolytic stressed conditions.
The mass balance was evaluated and is presented in table 2. Area for exclusion limit was established at 5500.
Mass balance of ketamine solutions after various stressed degradations.
No peaks of degradation products interfered with the peaks of lidocaine and ketamine. This affirmation is correlated with the peak purities evaluated with EZChrom Elite.
Chemical stability of solutions
HPLC assay
The percentage of lidocaine and ketamine remaining after storage at 28°C for various time points is shown in table 3. After 48 hours, both molecules retained more than 95% of the initial concentration.
Stability of lidocaine and ketamine diluted in 0.9% NaCl over time.
No peak of degradation product was detected during the course of the study.
pH measurements
pH measurements remained stable over the course of the study. The maximum of variation was 0.21 pH unit which is less than our acceptable limit.
Physical stability of solutions
Visual aspect
The solutions of lidocaine mixed with ketamine were clear and colourless. The colour of the solutions did not change over time. No precipitation or gas formation was noted during the study.
Subvisual aspect
The turbidity of the solutions at 550 nm was less than 0.010 AU for all three syringes for the duration of the study. The admixtures were physically compatible for 48 hours.
Discussion
Reversed phase HPLC
To evaluate the stability indicating capacity of the RP-HPLC method used, forced degradations of lidocaine and ketamine were realised and the mass balance was established for both drugs. The oxidative and alkaline degradations were the most effective for lidocaine. During the study, degrading ketamine with pH variations, heating or H2O2 addition was difficult. It has been previously described that ketamine is highly resistant to hydrolysis but sensitive to photolysis.13 Our mass balance correlates with this affirmation.
Stability study
One limit of our study was the subvisual assessment. Eur Ph 2.9.19 suggest two quantitative methods for the evaluation of non-visible particulates: Method 1 ‘Light obscuration particle count test’ and Method 2 ‘Microscopic particle count test’.14
These two methods allow the counting of the number of particles equal to or greater than 10 µm and 25 µm. Other analytical approaches in Eur Ph are presented in ‘2.2.1 Clarity and degree of opalescence of liquids’ which suggest two methods: nephelometry, which is the measurement of the light scattered by suspended particles, the measurement usually being made perpendicularly to the incident beam; and turbidimetry which is the measurement of the degree of attenuation of a radiant beam incident on particles suspended in a medium, the measurement being made in the directly transmitted beam.15
The International Pharmacopoeia specifies in the chapter ‘Physical and Physicochemical Methods, paragraph 1.10 Turbidimetry and nephelometry: 'Turbidity may be measured with a standard photoelectric filter photometer or spectrophotometer, preferably with illumination in the red-orange region of the spectrum (eg, by using a blue filter).’16
Turbidimetry and nephelometry have been used in numerous stability studies and Y-site compatibility studies to evaluate the subvisual aspect of physical stability.17 18 In our study, we have used turbidimetry at the visible wavelength 550 nm suggested by the European Guidelines for the practical stability studies.19
However, turbidimetry must be considered as a global measurement of particles suspended in a liquid and does not bring information on the size of the particulates. The Pharmacopoeia approach of paragraph 2.9.19 provides a better level of evidence for the non-visible evaluation of injectable solutions.
Lidocaine hydrochloride 20 mg/mL and ketamine hydrochloride 2.5 mg/mL diluted with 0.9% NaCl solutions retained respectively 99.98%±1.44% and 100.70%±0.95% after 48 hours' storage at 28°C in polypropylene syringes protected from light. The pH did not vary significantly during the course of the study. Therefore, the limit of stability of lidocaine with ketamine in these conditions is set to 48 hours. The effect of light was not evaluated in this study. The forced degradation realised showed that ketamine is highly sensitive to UV rays. Also, Lin AY et al 20 have highlighted that ketamine is sensible to photolysis in river waters.[20] However, Donnelly RF et al demonstrated that ketamine mixed with morphine was stable for 91 days of storage with exposure to light.13
Conclusion
The physicochemical stability of lidocaine 20 mg/mL and ketamine 2.5 mg/mL diluted with 0.9% NaCl in polypropylene syringes stored at 28°C protected from light was demonstrated for 48 hours. This infusion technique is therefore feasible from a pharmacologic point of view in burn-unit settings.
Key messages
What is already known on this subject
Admixture of lidocaine and ketamine may be used for opioid-free anaesthesia.
There is no stability data regarding this admixture.
Stability data is necessary to ensure patients’ safety.
What this study adds
Physicochemical stability was demonstrated for 48 hours.
This admixture is safe for use for opioid-free anaesthesia protocols.
Footnotes
EAHP Statement 3: Production and Compounding.
Twitter @fluidloading
Contributors BB: experiments performing, manuscript writing. DB: original idea, proofreading. JV: coordination, proofreading. BD: proofreading.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasoned request.