Article Text

Abstract
Objectives Medication non-adherence is common among patients with acute coronary syndrome (ACS) and is associated with poor clinical outcomes. To date, pharmacists have been underutilised in the delivery of adherence interventions. Across two studies, we assessed the feasibility, acceptability and effectiveness of a novel pharmacy-led intervention for patients hospitalised with ACS.
Methods The theory-based intervention was comprised of two personalised sessions addressing perceptual (negative/erroneous treatment beliefs) and practical (suboptimal action planning) barriers to adherence. Study 1: A single-arm, feasibility and acceptability study was conducted to determine proof-of-concept. Pre–post-comparisons using the Beliefs about Medicines Questionnaire-Specific (BMQ-S) were made. Study 2: A non-randomised controlled before–after pilot study was conducted with the intervention delivered by a team of clinical pharmacists. Follow-up data were collected at 6 and 12 weeks post-discharge. Primary outcome measures included the BMQ-S and the Medication Adherence Report Scale 5.
Results Study 1: 15 patients received the intervention and reported higher BMQ-S necessity scores post-intervention. The intervention was deemed highly acceptable to patients; therefore, further testing was sought. Study 2: A total of 56 patients were recruited: control (n=29) versus treatment (n=27). At 6-week follow-up, the treatment group had higher BMQ-S necessity scores (M=21.8, SD=3.1) compared with control (M=19.8, SD=2.7; p=0.045), although this effect was not maintained at 12 weeks. No differences were reported in the other outcome measures.
Conclusions Although the intervention was acceptable to patients, poor fidelity in delivery raises questions about its feasibility in practice. Furthermore, there was some impact on patients’ beliefs about medications but no effect on adherence. These findings demonstrate the importance of conducting feasibility and acceptability studies when developing adherence innovations in clinical care. Future studies should consider enhancing the training process to ameliorate fidelity issues.
- ischaemic heart disease
- clinical pharmacy
- quality in health care
- controlled trial
- myocardial infarction
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Medications are a central component of secondary prevention following acute coronary syndrome (ACS). Despite robust evidence supporting their efficacy when taken appropriately, approximately a third of patients do not adhere to medication following an ACS event.1 Non-adherence to cardiac medications is associated with a range of adverse outcomes including increased risk of mortality, revascularisation procedures and cardiovascular hospitalisations.2 Consequently, there is a need to better understand what drives adherence behaviour within this patient group and to develop strategies to support patients and healthcare providers (HCPs).
There is a growing literature drawing on theoretical models or conceptual frameworks to identify modifiable targets for adherence interventions. One such framework is the Perceptions and Practicalities Approach (PAPA) which posits that patient-level barriers to medication-use can be both perceptual, where beliefs shape an individuals’ motivation (ie, intentional non-adherence (INA); ‘those that won’t’), or practical, dictated by an individual’s ability, regardless of intention (ie, unintentional non-adherence (UNA); ‘those that can’t’).3 The PAPA has been proposed as a useful starting point when developing and evaluating adherence interventions.
Patients’ beliefs about their prescribed medications are a central tenet of the PAPA and can be conceptualised using the Necessity-Concerns Framework (NCF).3 The NCF proposes that a patient will weigh up the perceived need for treatment (necessity) against the potential for the treatment to cause harm (concerns) before deciding about whether to take the treatment or not. There is strong empirical evidence showing the utility of the NCF in predicting medication adherence in chronic conditions4 and in ACS specifically,5 although HCPs rarely address patients’ beliefs in routine practice.
UNA is common among patients with ACS6 which, according to the PAPA, relates to individuals lacking the ability to follow their treatment regimen as intended (eg, memory, dexterity, knowledge, organisation). Following ACS, patients are prescribed multiple medications; therefore, having a coherent medication-taking plan (ie, action plan) in place may reduce the likelihood of UNA (eg, forgetting doses). Implementation intentions are one particular action planning strategy which aims to link specific environmental cues with an intended behaviour or action (‘if situation X is encountered, then I will perform response Y’). Implementation intentions have been shown to reduce forgetting and improving medication adherence,7 although few adherence intervention studies for patients with ACS have used this strategy.8
Previous intervention studies in stroke9 and diabetes,10 explicitly targeting both intentional (eg, eliciting and modifying negative or erroneous treatment beliefs) and unintentional (eg, suboptimal action planning) barriers to non-adherence, have shown promising results. However, it is not yet known whether similarly designed interventions are feasible or effective when delivered by clinical pharmacists in routine practice. Within the UK’s National Health Service (NHS), recommendations from a 2016 Department of Health review of hospital efficiency has led to notable changes in hospital pharmacy practice in England.11 The report emphasised the need for clinical pharmacists to allocate more of their time working directly with patients on tasks relating to medicines optimisation, which includes promoting and monitoring adherence. Currently, there is a paucity of pharmacy-led adherence interventions which have been tested among cardiac patient populations, and in particular within hospital settings.8
Our aim was to therefore investigate the feasibility, acceptability and effectiveness of a brief, personalised, face-to-face intervention on patients’ beliefs about medications and self-reported adherence following ACS. Data are reported from two sequential studies: a feasibility and acceptability study (Study 1; NCT02967588); and a pilot study (Study 2; NCT03218813). This research was conducted in accordance with guidance from the UK’s Medical Research Council12 and reported in accordance with the Transparent Reporting of Evaluations with Nonrandomised Designs criteria13 (see online supplementary material 1.
Supplemental material
Study 1: feasibility and acceptability study
Methods
Design
Study 1 adopted a single-arm, pre–post-comparison design with the intervention delivered by a non-pharmacist (researcher; background in health psychology (JC)).
Setting and participants
Participants were recruited from the inpatient cardiology service at a large teaching hospital in central London, UK. This service includes a team of clinical pharmacists and pharmacy technicians who undertake ward-based, face-to-face consultations with patients. Routine clinical pharmacy practice comprises in-person medicines reconciliation and discharge medicines counselling. Participant inclusion criteria can be found in box 1. Recruitment took place between March 2017 and June 2017.
Participant inclusion criteria
Inclusion criteria
Adult patients (≥18 years of age)
Acutely admitted to hospital
Primary diagnosis of ACS (according to European Society of Cardiology Clinical Practice Guidelines) 33
Prescribed cardiovascular medicines (according to the UK’s National Institute of Health and Clinical Excellence guidelines: dual antiplatelet therapy; statin; β-blocker; angiotensin-converting enzyme [ACE] inhibitor/angiotensin II receptor blocker; glyceryl trinitrate spray) 34
No indication of cognitive impairment
Ability to read and understand English
Measures
Feasibility
Feasibility was assessed using participant uptake (% of eligible participants that consented) and retention (% of consented participants who completed the study) data. These metrics relate to the feasibility of conducting a trial of the intervention. Assessing the feasibility of the intervention in practice was addressed in Study 2.14
Acceptability
Acceptability was measured using scores from a purposely designed 10-item study feedback questionnaire (0–10 Likert scale). The tool measured ease of understanding, acceptability (setting, timing, content, delivery and deliverer) and perceived benefit. Participants were also invited to take part in semistructured telephone interviews in the weeks following discharge to provide additional feedback about the study. The interview guide was based on the items from the study feedback questionnaire.
Treatment beliefs
The Beliefs about Medicines Questionnaire-Specific (BMQ-S)15 comprises two 5-item subscales representing: (i) beliefs about the need for medication (necessity) and (ii) concerns about the risks of taking medication (concerns). Scores range from 5 to 25 on each subscale with higher scores indicating stronger beliefs. Both subscales have shown moderate internal consistency in a previous study of patients with acute myocardial infarction (necessity: α=0.80; concerns: α=0.68).16 A necessity-concerns differential score can also be calculated by subtracting the concerns subscale score from the necessity subscale score (range −25 to 25) with higher scores indicating more positive/adaptive beliefs about medication.
The intervention
The intervention comprised two personalised, face-to-face sessions delivered during an acute hospital admission for ACS. Session 1 focused on eliciting and challenging negative or erroneous beliefs about treatment and/or illness (ie, perceptual barrier) identified in a baseline screener questionnaire (see below). Session 2 focused on helping patients establish a coherent medication-taking routine (ie, overcome a practical barrier such as forgetfulness) using an implementation intention approach (eg, ‘If it is time X in place Y and I am doing Z, then I will take my pill dose’), which may also strengthen perceptual/intentional factors such as commitment to take medications and self-efficacy.17
The Behaviour Change Technique Taxonomy v1 (BCTTv1) was consulted to identify appropriate techniques which could be used in the intervention.18 A range of BCTs relevant to changing patient’s medication-taking beliefs and behaviour were selected from the BCTTv1 (see online supplementary material 2, table S1). The intervention was designed to complement routine clinical pharmacy care at the study site.
Supplemental material
Intervention tools
Screener
A self-report tool was designed to assess perceptual barriers to adherence. The tool comprised the 10-item BMQ-S15 along with four single-item questions (0–10 Likert scale) measuring treatment necessity (Necessity 1-item); concerns about treatment (Concerns 1-item); medication-related self-efficacy (Self-efficacy 1-item) and perceived illness duration (Timeline 1-item; taken from the Brief Illness Perception Questionnaire19), which has been shown to independently predict medication adherence among patients with coronary heart disease.20
Medicines planning sheet
Based on the method by Brown and colleagues,7 a Medicines Planning Sheet (MPS) was designed allowing patients to formulate and record medication-related implementation intentions. The MPS included examples of what an implementation intention should look like and provided templates to record plans for both morning and evening dosing.
Intervention process
On providing consent, participants completed a baseline screener questionnaire (pre-intervention). For Session 1, participant responses to the screener were reviewed and appropriate BCTs were selected based on issues that had been elicited. After completing Session 1, participants were left with the MPS and prompted to think about how medications would fit into their daily routine. For Session 2, participants were offered the opportunity to complete an MPS and rehearse their plans with the intervention deliverer. Participants retained a copy of their completed MPS. In most cases, Session 1 and Session 2 were delivered over consecutive days. For non-complex, short stay patients, both sessions were delivered the same day due to time constraints. Prior to discharge, participants completed another screener questionnaire (post-intervention) and a study feedback questionnaire (Study 1 only).
Statistical analysis
Statistical analysis was undertaken using IBM SPSS Statistics V.24. Shapiro-Wilk tests were conducted to determine normality of the data. Normally distributed continuous data were reported as means (M) and SD while not normally distributed continuous study variables were reported as medians (Mdn) and IQR. Pre-intervention and post-intervention BMQ-S scores were compared using paired samples t tests and Wilcoxon Signed Rank Tests for parametric and non-parametric data, respectively. For all analyses, a two-sided p value of 0.05 was considered statistically significant.
Results
Recruitment, uptake and retention
A total of 37 patients were considered for participation and 17 consented (45.9% uptake) (see online supplementary material, figure S1). Two participants who had consented withdrew before commencing Session 1, leaving 15 participants. All participants who commenced Session 1 completed both sessions. The mean duration for Session 1 and Session 2 was 30.3 min (SD=13.6) and 10.5 min (SD=7.6), respectively.
Supplemental material
Study sample
Details of the participant sample are shown in table 1.
Sample characteristics from Study 1
Outcomes
Acceptability
Scores on a study feedback questionnaire were high with a mean score of 9.5 out of 10 (SD=1.0) (see online supplementary material 2, table S2). Ten participants provided interview feedback (mean interview duration=12.3 min, SD=5.5). Generally, feedback from interviewees was positive with many highlighting benefits of taking part in the study (see online supplementary material 2, table S3).
Treatment beliefs
Patients’ beliefs about treatment were compared pre-intervention and post-intervention (see online supplementary material 2, table S4). BMQ-S necessity scores were significantly higher post-intervention compared with pre-intervention (t(13) = −3.36; 95% CI −3.05 o −0.66; p=0.005), with a large effect size (d=−0.90). There were also significant differences in post-intervention necessity-concerns differential scores (z=−2.94, p=0.003), with a medium effect size (d=−0.55). BMQ-S concern scores were lower post-intervention but this change was not statistically significant.
Based on these data, further testing of the intervention was sought.
Study 2: pilot study
Methods
Design
Study 2 adopted a non-randomised controlled before–after design with two cohorts of participants recruited over two sequential recruitment periods. The first cohort acted as the control group (‘before’) and the second as the treatment group (‘after’). A team of clinical pharmacists were trained to deliver the intervention between recruitment periods, thus creating two comparable groups.
Setting and participants
Participants were recruited from the same clinical setting using the same inclusion criteria described in Study 1. Recruitment took place between January 2018 and July 2018. Follow-up data were collected via post at 6-week and 12-week follow-up. A summary of the study outcomes is shown in table 2.
Outcome summary table from Study 2
Measures
Feasibility
As per Study 1, participant uptake and retention data were used to assess the feasibility of conducting a trial of the intervention.14 In addition, we were also interested in exploring whether the intervention was feasible in practice when delivered by the pharmacists (see Fidelity section).
Treatment beliefs
As per Study 1, the BMQ-S was used to measure patients’ treatment beliefs.
Medication adherence
The Medication Adherence Report Scale (MARS-5)21 is a 5-item scale that rates common non-adherence behaviours. Scores range from 5 to 25 where higher scores indicate higher medication adherence. The MARS-5 can be dichotomised into UNA (1-item) and INA (4-item) subscores and has shown good internal consistency among cardiac patient populations (α=0.92).22 A cut-off score of <25 was used to classify non-adherent vs adherent participants.6
Depression
The Patient Health Questionnaire-2 (PHQ-2)23 is a 2-item scale that briefly assesses the frequency of depressive symptoms over a 2-week period. Scores range between 0 and 6 with higher scores indicating more frequent depressive symptoms. A standard cut-off score of ≥3 is typically used to identify depression. The PHQ-2 is an internally consistent, validated instrument (α=0.83).24
Medicines-related information satisfaction
The Satisfaction with Information about Medicines Scale (SIMS)25 is a validated instrument assessing patients’ medication information needs. The SIMS comprises 17 statements across two subscales: ‘action and usage’ (AU) (9-item) and ‘potential problems of medications’ (PPM) (8-item). Higher scores indicate a high degree of overall satisfaction. Cronbach’s alpha values for the AU (α=0.93) and PPM (α=0.89) subscales have shown good internal consistency among cardiac inpatients.26
Medicines-related self-efficacy
The Self-Efficacy for Appropriate Medication Use Scale (SEAMS)27 comprises 13 items. Total scores on the instrument range from 13 to 39 with higher scores reflecting greater confidence in the responder’s ability to adhere to treatment. The instrument has been shown to have good internal consistency (α=0.89).27
Sample size
A power calculation using Study 1 necessity-concerns differential data (see online supplementary material 2, table S4) indicated that a sample of 55 participants in each group would be sufficient to detect a medium effect of the intervention. Adjusting for an estimated attrition rate of 20%, the target sample size was 66 participants per group (n=132).
Pharmacy training package
A 90 min interactive training workshop was delivered by the researcher who conducted Study 1 (JC). The first half of the workshop was dedicated to the clinical pharmacy team familiarising themselves with the intervention tools and processes while the second half involved role play. A total of 14 pharmacists/pharmacy technicians received training. The researcher also remained on-site in a support role for the duration of the study period to facilitate recruitment and aid the clinical pharmacy team where necessary. The researcher did not conduct any intervention sessions during Study 2.
Fidelity
An Intervention Checklist was designed so that pharmacists could document the content of their intervention sessions (eg, problem identification, BCTs used, reflections) to help standardise and monitor delivery. They were asked to retain completed Intervention Checklists for the researcher to review for fidelity purposes. These data would help determine whether it would be feasible for the intervention to be used in practice.
Statistical analysis
Descriptive data reporting and univariate analyses were the same as in Study 1. Baseline comparisons between groups were made using independent samples t-tests, χ2 tests or Mann-Whitney U tests. A repeated-measures analysis of variance was used to compare changes in outcome measures over time and between groups. Group × time interactions were also calculated.
Results
Recruitment, uptake and retention
A total of 56 participants were recruited which equates to 42.4% of our target sample size (n=132) (see figure 1). The uptake rate in the treatment group (47.4%) was comparable to Study 1 (45.9%). Intervention duration was recorded for 12/27 participants (M=17.7 min, SD=7.8). Nine members of the clinical pharmacy team—eight pharmacists and one pharmacy technician— delivered at least one intervention. The pharmacy team did not routinely use Intervention Checklists which indicates fidelity issues.

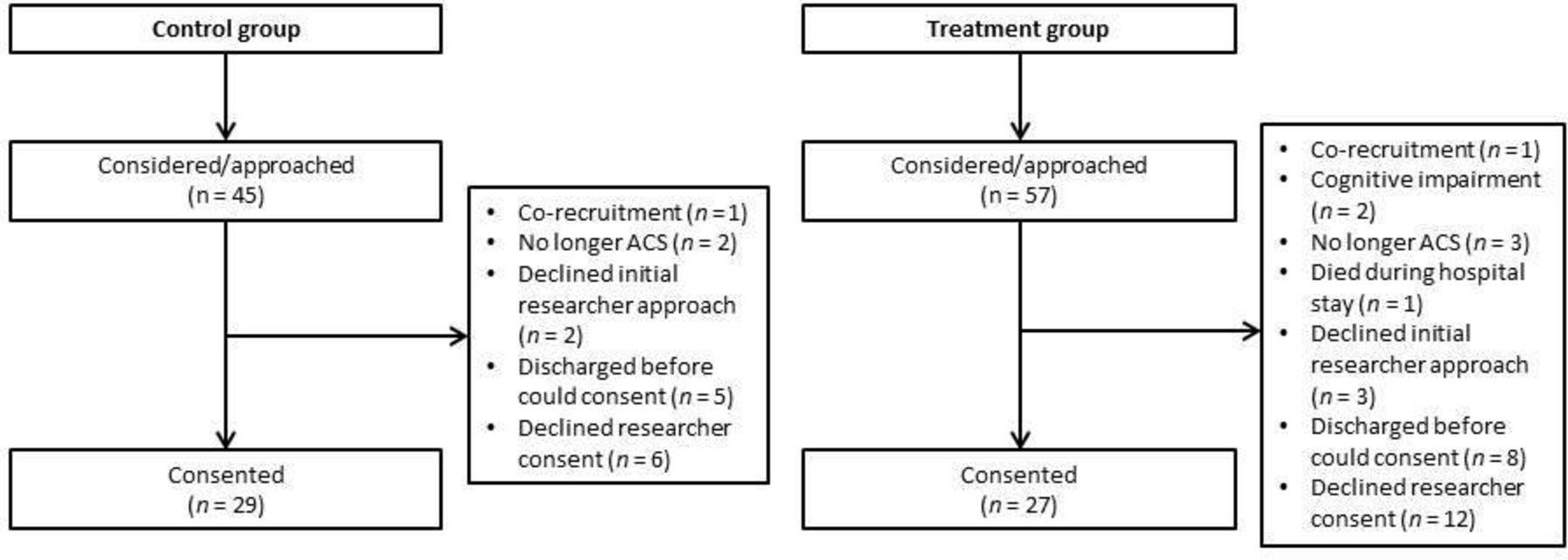{kind=link}
Participant flow diagram for Study 2.
Study sample
Details of the participant sample are shown in table 3. Overall, demographic and clinical factors were similar between groups.
Sample characteristics from Study 2
Outcomes
Treatment beliefs
BMQ-S necessity scores favoured the treatment group at 6-week follow-up (U=141.0, p=0.045), although this effect was not maintained at 12-week follow-up (U=166.5, p=0.263) (see table 4). There were significant main effects of time for BMQ-S necessity (F=3.68, p=0.024), BMQ-S concerns (F=8.06, p=0.001) and necessity-concerns differential scores (F=13.65, p=0.001). BMQ-S concerns showed a significantly greater decrease over the follow-up period in the treatment group versus control group (F=3.30, p=0.035). Necessity-concerns differential scores also showed a significantly greater increase by follow-up in the treatment group compared with control (F=3.62, p=0.026).
Group comparisons for treatment beliefs and medication adherence from Study 2
Medication adherence
The intervention had no effect on MARS-5 scores between groups (see table 4). A total of 38.1% and 28.6% or participants reported non-adherence (MARS-5 <25) at 6 weeks in the control and treatment groups, respectively (χ² (1, n=42)=4.29, p=0.513). At 12 weeks, 22.7% of control group participants and 40.0% of treatment group participants reported non-adherence (χ² (1, n=42)=1.46, p=0.227).
Depression
At baseline, approximately one in five participants met the standard PHQ-2 cut-off score for depression (≥3) (control 17.9% vs treatment 23.1%). At 12-week follow-up, this number was lower in both groups (control 13.6% vs treatment 5.0%). There were no group differences in depression at baseline (χ² (1, n=54)=0.23, p=0.634) or 12-week follow-up (χ² (1, n=42)=0.907, p=0.341).
Medicines-related information satisfaction
There was no group differences for pre-discharge SIMS total score (control: Mdn=13.0, IQR=7.0 vs treatment: Mdn=15.0, IQR=5.8, U=221.5, p=0.237), AU subscale score (control: Mdn=9.0, IQR=3.0 vs treatment: Mdn=9.0, IQR=1.0, U=224.5, p=0.209) or PPM subscale score (control: Mdn=5.0, IQR=4.0 vs Mdn=6.5, IQR=4.5, U=227.5, p=0.290).
Medicines-related self-efficacy
There was no difference in 12 weeks SEAMS score between the control group (Mdn=35.0, IQR=8.0) and treatment group (Mdn=34.5, IQR=7.0), U=218.0, p=0.960.
Discussion
This paper reports the initial evaluation of a brief, personalised, face-to-face intervention on patients’ beliefs about medications and self-reported adherence following ACS.
Study 1 revealed that the intervention, when delivered by a non-pharmacist, was deemed acceptable to patients in terms of setting, delivery, timing, content and deliverer. Feedback from post-discharge interviews was generally positive with participants highlighting benefits of taking part. That being said, study uptake was relatively low (45.9%); however, this was often due to practical factors (eg, insufficient time to complete) rather than patients declining. In terms of effectiveness, our self-report data revealed that patients’ beliefs about medications had become more positive/adaptive after receiving the intervention.
The aim of Study 2 was to explore whether the intervention could be successfully delivered by a team of clinical pharmacists, who had undergone training to deliver it. It must, however, be noted that these data should be interpreted with caution because of suboptimal recruitment to the study (achieved 42.2% of target). Patients receiving the intervention had stronger necessity beliefs after 6 weeks compared with control; however, this effect was not maintained at 12 weeks. The intervention also had no effect on rates of self-reported medication adherence, which was rated high in both groups. These findings mirror those from two previous pharmacy-led interventions which found that changes in patients’ beliefs did not translate into improved adherence to cardiac medications.28 29
There are several possible reasons for these findings. First, the study lacked power due to suboptimal recruitment. Slow recruitment during trials is common which reinforces the need to undertake feasibility and acceptably assessment. The uptake rate was similar to Study 1 which supports the notion that the setting and timing of the intervention made recruitment challenging. For example, hospital stays of non-complex ACS cases can be short, which leaves a narrow window for all the components of the intervention to be delivered in a busy clinical setting.
Second, the study was likely hampered by fidelity of delivery issues. Despite having a fidelity protocol in place (eg, Intervention Checklist), pharmacists’ compliance to this protocol was poor. Intervention sessions were shorter in Study 2 compared with Study 1 which suggests that the pharmacy-led sessions may have been rushed. As such, it is questionable whether it would be feasible for the intervention to be used in practice. Further evaluation and advancement of this intervention should prioritise having a stringent feasibility protocol is in place to ensure accurate delivery (eg, observation and feedback, audio recording sessions9 10).
Third, it was only possible to offer a single 90 min training session to up-skill the clinical pharmacy team which may not have been long enough to engage and educate the team to the level required to stimulate practice change. Although the training session was interactive and included role play, additional strategies, such as those involving video recorded consultations and feedback,30 could have also been employed. Additional feasibility and acceptability work with future intervention deliverers would be useful to identify their training and support needs to maximise engagement going forward. This would also likely benefit intervention fidelity.
Fourth, it may be that routine pharmacy care was of high quality at the study site. Patients admitted at the study site would typically consult with the pharmacy team at least twice during their hospital stay (ie, medicines reconciliation and discharge counselling). However, this level of pharmacy contact is not universal across acute NHS settings.11 It is conceivable that our intervention may be more effective in settings where patients do not routinely see a clinical pharmacist during their hospital stay.
Fifth, participants were not screened for low adherence on entering the study. While there are often practical reasons for this, interventions targeting poor medication adherers have been shown to be more effective compared with interventions delivered to all medication-takers.31 Future studies should therefore consider focusing on delivering interventions to individuals who may benefit the most from them.
Over the years, various theories and models of health behaviour have been proposed to help explain the mechanisms driving medication-taking behaviour. By understanding these mechanisms, it is possible to identify modifiable targets for behaviour change interventions. This intervention applied the PAPA to target medication adherence in patients with ACS. While the PAPA is useful to identify what needs to be targeted (perceptual barriers vs practical barriers), it does not advise about which strategies work best to change actual behaviour. Additional steps must be taken to achieve this. For this intervention, we used the BCTTv1 to help identify suitable BCTs to elicit and modify our target behaviour. Although the identification and selection of appropriate BCTs was done intuitively, there is a need to develop robust and replicable methods of selecting the most effective BCTs or BCT combinations to target specific behaviours in specific contexts.32
Conclusion
Initial testing of a brief intervention, addressing patients’ beliefs about medications to reduce INA in conjunction with an implementation intention approach to reduce UNA, was deemed to be highly acceptable by patients, but had no effect on rates of self-reported adherence following ACS. There were several design and methodological issues which likely contributed to these findings, which highlights the importance of conducting early-stage feasibility and acceptability research before embarking on large trials. Further evaluation and advancement of this intervention should focus on the best way to train pharmacists to deliver this type of intervention along with monitoring fidelity of delivery more closely.
What this paper adds
What is already known on this subject
Medication non-adherence is common among patients with acute coronary syndrome (ACS), resulting in poor clinical outcomes.
It is important to identify modifiable barriers to medication-taking early on following ACS.
Few adherence interventions have been theory-based and have utilised pharmacists in their delivery.
What this study adds
Study 1 suggests that a brief, hospital-based intervention was deemed acceptable to patients receiving it.
Study 2 suggests that when the intervention was delivered by a team of pharmacists, there was limited impact on patients’ beliefs about medications and no impact on self-reported adherence.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was granted by London - Chelsea NHS REC (17/LO/1706).
Acknowledgments
The authors would like to thank the patients who took part in this study. We would also like to express our gratitude to the pharmacy team for their participation and, in particular, Imran Hafiz who helped coordinate this research project
References
Footnotes
EAHP Statement 4: Clinical Pharmacy Services.
Contributors JC, JW, DM and VA were involved in the study conception and design. JC led data collection and analysis. All authors approved the final manuscript.
Funding This work was supported by a King’s College London – University of California, San Francisco four-year full-time PhD studentship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.