Article Text

Abstract
Objectives Norepinephrine is a vasopressor frequently administered after dilution to treat hypotension and shocks in intensive care units. The stability of norepinephrine is known to be highly sensitive to storage conditions. Moreover, medication errors linked to the dilution step are frequent and may be deleterious for critically-ill patients, especially in intensive care units. This study aimed to evaluate the stability of ready-to-use diluted norepinephrine solutions prepared at two target concentrations (0.2 and 0.5 mg/mL), according to the summary of product characteristics, and stored for 365 days in two containers: AT-closed cyclic olefin copolymer vials, and polypropylene syringes.
Methods A fast reversed-phase liquid chromatography method coupled with an ultra-violet detector was developed to assess the chemical stability of norepinephrine solutions. Validation was conducted according to the linearity of the calibration ranges, selectivity, sensitivity, accuracy and precision. Dosage, sub-visible particle contamination, pH monitoring and sterility assays were performed. Chemical stability was maintained if the measured concentration respected the lower limit of 90% of the initial concentration. Containers were stored at −20±5°C, +5±3°C and +25±2°C with 60±5% relative humidity in a dark closed enclosure.
Results Stability was successfully maintained for every concentration and container tested when stored at −20±5°C and +5±3°C. In these storage conditions, particle contamination, pH monitoring and sterility assay respected the required criteria. Chemical degradation and colouring of solutions appeared before the end of the 1 year study period for most norepinephrine solutions stored at room temperature.
Conclusions Ready-to-use solutions containing 0.2 and 0.5 mg/mL norepinephrine in polypropylene syringes or cyclic olefin copolymer vials must be stored at refrigerated or frozen temperatures to obtain acceptable 1 year shelf-stability. Exposure to higher temperatures significantly decreases shelf-stability. Our study protocol for compounding polypropylene syringes and cyclic olefin copolymer vials containing norepinephrine is adapted to implementation in centralised intravenous additive services.
- drug stability
- intensive & critical care
- IV administration
- shelf life
- validation analytical procedure
Statistics from Altmetric.com
Introduction
Norepinephrine (NE) is a vasopressor frequently administered to treat hypotension and shocks in intensive care units (ICUs).1 In France, injectable bitartrate NE solutions are available at 0.5 and 1 mg/mL packaged in 50 mL vials and 2 mg/mL in 4 or 8 mL vials. The product monographs recommend diluting 0.5, 1 and 2 mg/mL solutions with 5% dextrose (D5W) or 0.9% sodium chloride (normal saline solution, NS). Medication errors linked to the dilution step are frequent and may be deleterious, especially for critically-ill patients in ICUs.2–5 Compounding in hospital pharmacies provides qualitative injectable solutions and avoids the dilution step in the ward.6 The stability of NE is known to be highly sensitive to storage conditions7 and the 365 day stability of 0.2 mg/mL and 0.5 mg/mL solutions of NE diluted in NS and stored in polypropylene (PP) syringes or cyclic olefin copolymer (COC) vials has never been assessed before.8–17
The objective of this study was to evaluate the stability of two concentrations (0.2 mg/mL, 0.5 mg/mL) of NE diluted in NS and stored for 365 days at frozen (−20±5°C), refrigerated (+5±3°C) or room temperatures (+25±2°C) in two ready-to-use storage containers: PP syringes and COC vials.
Methods
Products
NE standard reference used for the validation step was prepared based on the NE commercial solution (Noradrenaline Mylan 2 mg/mL sans sulfites, Mylan, Paris, France). Phosphate buffer 20 mM, prepared with monopotassium phosphate (Cooper, Melun, France) diluted in ultra-pure water (ELGA LabWater, Antony, France), 85% orthophosphoric acid and acetonitrile (VWR International, Fontenay-sous-Bois, France), were used for the mobile phase. Containers for the study were 20 and 50 mL PP syringes (Plastipak, Becton Dickinson, Le Pont-de-Claix, France) and 20 and 50 mL AT-closed vials (Aseptic Technologies, Gembloux, Belgium).
Containers
The AT-closed vials were designed to provide users with clean, hermetically closed, sterile, ready-to-fill and ready-to-use containers. Their body was made of COC and the stopper of thermoplastic elastomer. Mechanical resistance and high transparency are the two main characteristics of COC. The fully automated vial manufacturing process18 ensures aseptic conditions and meets the required criteria defined for pharmaceutical primary containers in the US Pharmacopoeia (USP): USP 87—in vitro toxicity on cells for both vial body and stopper; USP 88—in vivo toxicity for both vial body and stopper; USP 661—physicochemical tests for the vial body.
Standard solutions
Two calibration curves were made in triplicate using five levels of standards (curve A: 0.12, 0.16, 0.20, 0.24, 0.28 mg/mL; curve B: 0.3, 0.4, 0.5, 0.6, 0.7 mg/mL) based on the NE commercial solution (2 mg/mL) diluted in NS. Standards were injected into the system without dilution.
Solution preparations
Both concentrations were tested in different containers. The stability of 0.2 mg/mL NE solutions was tested in 20 mL and 50 mL containers: 150 syringes and 300 COC vials of each volume. The stability of 0.5 mg/mL NE solutions was only tested in 50 mL containers: 150 syringes and 300 COC vials. The PP syringes were filled manually by two pharmacists. Stock solutions were prepared by diluting the commercial solution in NS plastic containers (Viaflo, Baxter, France), following the removal of excess NS solution. A needle-free medical device for administration (PCHIMX, Doran International, France) was used to fill the PP syringes.
The COC vials were filled through an M1 Filling Station (Aseptic Technologies, Gembloux, Belgium) connected to a peristaltic pump (Flexicon Pump PF6, Watson Marlow, La Queue Lez Yvelines, France).19
Storage conditions
Half of the COC vials were stored upright and the other half upside-down. The objective of upside-down storage was to evaluate the effect of the stopper on the stability of the preparation by ensuring contact between the NE solution and the stopper throughout the study period.
All PP syringes and COC vials were stored in the dark, in hermetically closed enclosures at −20±5°C,+5±3°C and +25±2°C with 60±5% relative humidity (RH). Frozen samples were defrosted for 4 hours at room temperature just before chromatographic analysis. Each vial and each syringe was used once for analysis without dilution.
Chromatographic apparatus and conditions
A reversed-phase fast liquid chromatography (FLC) system (Agilent 1260 Infinity LC, Les Ulis, France) equipped with an Apollo C18 Alltech column (5 µm, 250 mm × 4.6 mm, Grace, Epernon, France) maintained at +25°C coupled with an ultra-violet (UV) detector (1260 MWD DEAAZ00942) was used to measure NE concentrations. The wavelength was set at 279 nm.9 The injection volume was 5 µL for all analyses. A mobile phase A/B 97/3 (v:v) with isocratic elution was used consisting of (a) 20 mM phosphate buffer/orthophosphoric acid, pH adjusted at 2.5, and (b) acetonitrile. The flow rate was fixed at 1 mL/min. ChemStation software (OpenLab CDS, version 01.05) piloted the system.
Forced degradation study
Conditions to obtain about 20% of the initial amount of NE were:
Acidic: hydrochloric acid 1N, (VWR International) at room temperature for 30 min, then neutralisation with NaOH 0.01N (VWR International)
Basic: NaOH 0.01N at room temperature for 30 min, then neutralisation with HCl 0.1N
Heat: storage in a heated chamber (Binder ED 115, Tuttlingen, Germany) at +70°C for 3 days.
Oxidative: H2O2 at 30% (Gilbert, Hérouville Saint-Clair, France) for 1 day
Light: exposure to UV light (Mineralight Lamp UVSL-25, 24 W, Ultra-violet Products Inc, San Gabriel, California) for 2 days.
Once the forced degradation study was over, the degradation solutions were diluted with the mobile phase to a 0.5 mg/mL concentration before injection into the HPLC (high-performance liquid chromatography). The chromatogram of NE commercial solutions was compared with those obtained from the forced degradation solutions.
Dye ingress test
A methylene blue (MB) test was performed in triplicate to assess the hermetic seal of each container filled with 50 mL NS and stored at the three temperatures. After 365 days of storage, each container was submerged for 2 min in a bath of 1 g/L MB solution at ambient temperature and atmospheric pressure. The examination of colouring was performed with unaided eye.
Operating conditions for the stability study
The stability-control process was conducted respecting International Council of Harmonisation (ICH-Q1A) guidelines20 and SFPC/GERPAC recommendations.21
The stability of 0.2 and 0.5 mg/mL NE solutions was assessed at 14 time points (days 0, 1, 2, 3, 4, 7, 14, 21, 28, 60, 90, 180, 270, 365) by visual inspection, by measuring NE concentration and by pH monitoring. The particulate contamination test and sterility assay were performed at the beginning and end of the stability study.
The visual inspection analysis included colouring, transparency of the solution and formation of visible particles. Chemical stability was assumed to be maintained if no toxic degradation product was formed and if the measured concentrations were >90% of the initial concentration and with no colour change.21 pH values were measured in triplicate with a Hanna HI 223 pH-metre (Hanna Instrument, Michigan, USA) for all conditions.
The non-visible particulate contamination assay was performed using a light obscuration spectrometer (APSS-2000, Particle Measuring System, Dourdan, France). The acceptance thresholds were fixed at 6000 for particles of sizes ≥10 µm/container and 600 for particles of sizes ≥25 µm/container.22 To conduct the sterility test, samples were filtered using membranes with a 0.45 µm cellulose nitrate filter (Sartorius Stedim Biotech, Göttingen, Germany), which were incubated at +35°C in a fluid thioglycollate medium and at +22°C in a soya-bean digest casein medium for 14 days.23
Statistical tests
For the calibration curves, we plotted the peak area obtained for the calibration solutions of NE versus the concentrations of NE contained in those solutions. The linearity of our method was assessed through a Cochran test with non-significant results followed by an analysis of variance (ANOVA).
Intra-day precision was assessed by analysing in triplicate samples prepared on the five concentration levels for the two calibration ranges; inter-day precision was assessed by repeating the same analyses of the same samples on three consecutive days. The recovery factor was used to calculate accuracy and the coefficient of variation to evaluate the precision of the stability-indicating method. Total error was calculated as the sum of relative bias and inter-day precision.
The pH values obtained from storage in the three different containers were compared at day 0 (n=3) and day 365 (n=3) over the 27 different conditions (R software, version 3.6.1) using a non-parametric Wilcoxon test (α=0.05).
Results
Dye ingress test
According to the results (online supplementary data table 1), the seal of each container was assumed to be hermetic.
Supplemental material
Forced degradation study
The representative chromatograms of the commercial 2 mg/mL NE solution diluted in NS at 0.5 mg/mL and those obtained from the degradation study are presented in figure 1. NE was eluted at 3.2±0.0 min with a symmetry peak factor respecting European Pharmacopoeia (EP) criteria (symmetry factor=1.16, reference standards=0.8–1.5). Degradation under basic conditions led to the formation of a product eluted at 2.6 min while degradation under acid conditions yielded three products eluted at 3.6, 4.0 and 4.4 min. Dilution with H2O2 30% led to the formation of two degradation products eluted at 4.1 and 6.6 min. Exposure to heat resulted in the formation of two degradation products (4.0 and 4.7 min). Exposure to UV light revealed no degradation products. There was no interference between peaks of the NE and those of the degradation product.

Representative chromatograms of: (A) 0.5 mg/mL norepinephrine (NE) solution diluted in 0.9% NaCl; (B) 0.5 mg/mL NE solution diluted in 0.01N NaOH; (C) 0.5 mg/mL NE solution diluted in 1N HCl; (D) 0.5 mg/mL NE solution diluted in H2O2 30%; (E) 0.5 mg/mL NE solution stored in a heated enclosure.
Validation assay for both 0.2 and 0.5 mg/mL NE solutions
Validation data for the two calibration ranges are summarised are table 1.
Validation parameters for the two calibration ranges
According to these results, these two calibration ranges have high linearity. The accuracy and inter-day precision of both calibration ranges are presented in table 2.
Results of accuracy and inter-day precision for the two calibration ranges: A for the 0.2 mg/mL concentration; B for the 0.5 mg/mL concentration
Concerning total error and accuracy, the results were within the expected limits (<10% and between 90–100%, respectively). Linearity, sensitivity, selectivity, precision and accuracy were successfully demonstrated for our physicochemical NE stability-indicating method.
Physicochemical stability of NE
Before storage, the prepared solutions were clear, without any visible particles. The pH values measured were 3.35±0.03 (n=9) for 0.5 mg/mL and 3.60±0.00 (n=9) for 0.2 mg/mL NE solutions.
At the end of the study period, solutions compounded in containers maintained at −20±5°C and +5±3°C were clear, colourless and without any visible particles. However, a greyish-brown colouring appeared on day 90 in the PP syringes and on day 120 in COC vials, for both concentrations stored at +25°C and 60% RH.
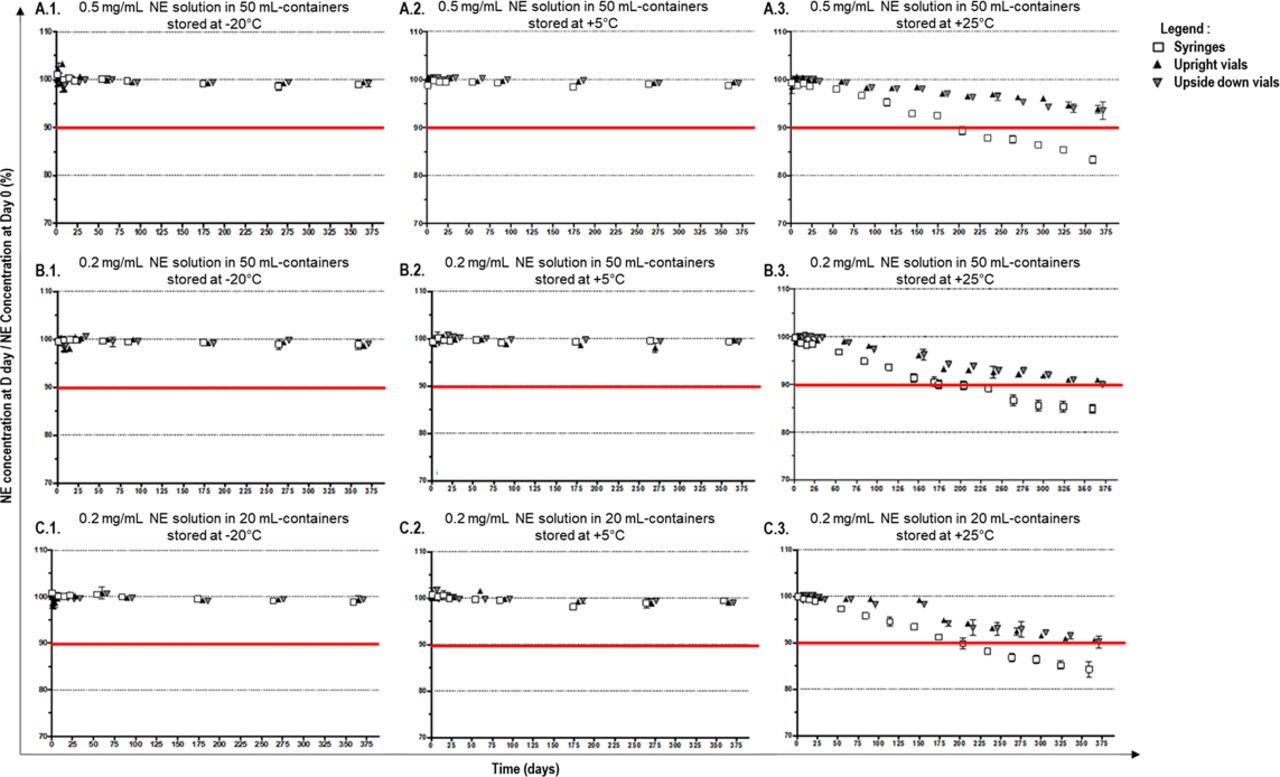
The results obtained from the stability assay for every concentration, container and temperature condition tested are summarised in figure 2 and online supplementary file 4.
Supplemental material

{kind=link}
{kind=link}
Results of the stability assay for 0.2 and 0.5 mg/mL norepinephrine (NE) solutions (n=3).
Results showed that chemical stability was maintained over the 365 day study period for 0.2 mg/mL NE solutions and 0.5 mg/mL NE solutions whatever the container when the storage temperature was −20±5°C and +5±3°C. Stability was also maintained for 0.5 mg/mL solutions stored in upside-down and upright vials and 0.2 mg/mL NE solutions stored in upright 50 mL vials at +25°C and 60% RH. However, stability after storage at +25°C and 60% RH was maintained until:
day 150 for 0.2 mg/mL NE solutions in 50 mL PP syringes
day 180 for 0.2 mg/mL NE solutions in 20 mL PP syringes
day 330 for 0.2 mg/mL NE solutions in 50 mL upside-down vials, for 0.2 mg/mL solutions in 20 mL upside-down and upright vials.
Particle contamination, pH and sterility
Particle contamination at day 0 reached the required EP criteria. This assay was not performed at day 365 for containers stored at +25°C and 60% RH as solutions became coloured from day 90 (syringes) or day 180 (vials). The results for particle counting at day 365 for containers stored at −20±5°C and +5±3°C are summarised in online supplementary data table 2 and reached the limits determined by EP specifications. pH values measured at day 0 and day 365 are presented in online supplementary data table 3. No difference in pH values was noted between the beginning and the end of the study (Wilcoxon test, p>0.05).
Supplemental material
Supplemental material
Sterility remained constant throughout the study period whatever the container, the storage conditions and the NE concentrations (0.2 or 0.5 mg/mL) tested.
Discussion
A stability-indicating HPLC-UV method to determine the physicochemical stability of NE bitartrate hydrochloride injectable solutions was successfully designed and validated. Our study showed that stability was maintained for 365 days in PP syringes and COC vials when stored at −20±5°C and +5±3°C.
The long-term stability of 0.2 and 0.5 mg/mL NE solutions diluted in NS in PP syringes and ready-to-use-COC vials had not been investigated before. The closest in terms of study design assessed the stability of 0.1, 0.2, 0.4 and 0.04 mg/mL NE solutions in amber glass vials, and 0.01 mg/mL NE solutions diluted in D5W stored in 10 mL PP syringes for 12 months at +2°C to 8°C and ambient temperature.15 Results were partly comparable with ours as the stability of 0.1, 0.2 and 0.4 mg/mL solutions was maintained over the study period when stored refrigerated. However, NE injection solutions, 0.01 mg/mL in 10 mL PP syringes, were seen to be stable for only 6 months when stored refrigerated and 28 days when stored at ambient temperature. Previous studies successfully assessed the stability of NE solutions over shorter periods,9–14 with storage at ambient9 11–13 or refrigerated9 14 temperatures, in polyvinyl chloride bags,9 11 13 14 PP syringes,12 with dilution in NS9 11 or D5W,9 11–14 exposed to9 11 12 or protected from9 12–14 light, with different NE concentrations. The NE commercial solution used for our stability assay was devoid of antioxidative stabilising agents.
The degradation pathways of catecholamines via their oxidative reaction responsible for colouring have been widely described.24 Oxidation leads to the formation of noradrenochromes15 which account for the greyish-brown colour. This oxidative process is catalysed by oxygen, heat, alkalinisation with a pH value >6, heavy metal ions, and exposure to UV or daylight.14 16 17 The analogues and metabolites of noradrenochromes have been reported as being neurotoxic and cardiotoxic in the literature.25 No acceptance limits have been defined regarding the content of degradation products in current NE monographs.26 In the chromatograms of the degraded solutions, we identified one peak corresponding to the formation of a degradation product at 4.0±0.1 for a 0.2 mg/mL NE solution stored in 20 mL and 50 mL, and two peaks corresponding to the formation of two degradation products at 3.8±0.0 min and 4.3±0.0 min for an NE solution stored in 50 mL. According to our forced degradation study, these peaks could be assimilated to the degradation compounds eluted at 3.6 and 4.4 min in acid conditions.
The sensitivity of catecholamine degradation to light has previously been shown,15 27 but it could not be responsible for the NE degradation in our study because each container tested was stored in a closed enclosure. Other studies have assumed that the major determinant of the degradation process is pH.16 Our initial pH values (3.30–3.60) were within the limits recommended.27 As the degradation products identified in the degraded solutions were also identified in acid forced degradation conditions, a very slight variation in pH might be one of the factors catalysing the degradation process. Finally, many converging arguments have forced us to assume that temperature plays a major role in catalysing the degradation process of NE, as sub-visible particulate contamination was low when stored in frozen and refrigerated conditions while solutions stored at ambient temperature became coloured. The assumption that stability is prolonged with refrigerated or frozen storage has already been raised,9 10 and many studies have successfully used freezing to lengthen drug stability. Protocols using microwaves for defrosting have also been published.
Our results also support the claim that COC vials offer longer stability than PP syringes since the colouring of solutions was delayed by 1 month when stored in the former.
The strong point of our study lies in the implementation of ready-to-use containers. The COC vials provide an original design for a high-quality container28 meeting the criteria of authority requirements for pharmaceutical primary containers. The safety and efficacy of COC vials to maintain the long-term stability of injectable solutions have previously been demonstrated.18 The counting of sub-visible particles is another strong point, as this was not performed in previous stability studies.8–13 15–17
Variability in solution concentrations prepared at the patient’s bedside is a major issue.3 This inter-operator variability can result in the administration of under- or over-concentrated solutions with adverse effects, especially in the case of high-risk medication.15 Preparing injectable solutions at the patient’s bedside is also a microbiological challenge.7 The centralised preparation of ready-to-use solutions would undeniably improve the security of parenteral administration but requires time-demanding organisation. To this end, fast methods of dosage need to be developed for routine use. Several methods with reversed-phase HPLC combined with UV detection have been developed in previous studies.9 We also chose UV to detect degradation products as the main degradation products of NE contain chromophores in their chemical structure, as previous studies have shown.7 This method is compatible with routine practice and more common than other methods (ie, electrochemical detection10 11 or photodiode array detection12 15).
The compounding of ready-to-use syringes and COC vials raises the question of how a single-dose protocol in ICU services should be defined, as the prepared ready-to-use solutions are compounded to be administered as such. Analyses have not been pursued beyond the date originally envisaged for the end of the study as 365 day stability is sufficient to provide ICUs with ready-to-use solutions in routine practice. During our assay, we did not seek to identify leachables and extractables from the COC as such tests have previously been performed and confirmed the low risk of COC packaging.18 The PP syringes in our study were not designed for aqueous drug storage although this is regular practice in ICUs. Our stability assay took place before the US Food and Drug Administration alert to healthcare professionals not to administer compounded drugs stored in Becton Dickinson (BD) syringes (2015). More recently, BD has announced that it is no longer using material associated with a loss of drug potency, so that their syringes are now suitable for storing compounded drugs.29
Conclusions
Considering our results, ready-to-use solutions containing 0.2 and 0.5 mg/mL NE in PP syringes or COC vials need to be stored at refrigerated or frozen temperatures to have acceptable 1 year shelf-stability. Exposure to higher temperatures significantly decreases shelf-stability. According to our study protocol, the compounding of PP syringes and COC vials containing NE is adapted to implementation in hospital pharmacies.
What this paper adds
What is already known on this subject
Medication errors linked to the dilution step are frequent and may be deleterious for critically-ill patients especially in intensive care units.
The stability of norepinephrine (NE) is known to be highly sensitive to storage conditions.
Compounding in a hospital pharmacy avoids the dilution step in the ward by providing safe ready-to-use solutions.
What this study adds
The storage of ready-to-use solutions containing 0.2 and 0.5 mg/mL NE in polypropylene (PP) syringes or cyclic olefin copolymer (COC) vials, at refrigerated (+5±3°C) or frozen temperatures (−20±5°C), in the dark, offers acceptable 1 year shelf-stability.
Storage of ready-to-use solutions at higher temperatures (+25±2°C) significantly decreases the stability of NE solutions by up to 2 months when compounded in PP syringes or 3 months in COC vials.
COC vials offer longer stability than PP syringes for the storage of NE solutions.
Acknowledgments
We thank Alexandra Tavernier (MA, University of Glasgow, Professeur Agrégée, France) for English language and editing assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
EAHP Statement 3: Production and Compounding.
Twitter @Sixtine Gilliot, @MorganeMasse
Contributors SGi contributed to formal analysis, writing, reviewing and editing of the final version. MM contributed to formal analysis, reviewing and editing of the final version. SGe contributed to the study conception, data curation, methodology, validation and revision of the final version. DL, CB, BD and PO contributed to supervision, methodology, validation and revision of the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are available in the data repository, uploaded with the article.