Article Text

Abstract
Objectives As part of the service provided by clinical pharmacists in our hospital, an assay for plasma amikacin quantification by liquid chromatography-tandem mass spectrometry (LC-MS/MS) has been established for clinical use since 2018. This study was undertaken to describe: (1) the establishment of this assay; (2) the application and results of the testing; and (3) the analysis and impact for patients.
Methods The amikacin quantification assay was validated and the plasma amikacin concentration data were extracted and analysed. The clinical data for related patients were collected from electronic health and medical records.
Results 121 plasma samples from 53 patients were included in this statistical analysis. The use of amikacin was mostly monitored in the intensive care unit and the haematology department, and the monitoring range of amikacin concentrations were about 0.1–57µg/mL. The main indications for amikacin concentration detection were combined medications, impaired renal function, or people over 65 years old, which may increase the incidence of adverse reactions. Amikacin prescribing decisions were diversified due to the combination of assay results and clinical disease progression, and the effective rate of amikacin administration was about 52.8% (28/53).
Conclusions The assay for plasma amikacin concentration has been successfully established to monitor the clinical use of amikacin, and the assay results served as one of the references for amikacin prescribing decisions.
- therapeutic drug monitoring
- pharmacy service
- hospital
- administration
- intravenous
- analytic sample preparation methods
- clinical laboratory techniques
Data availability statement
The data were collected in the database of a third party which were not publicly available due to the patient privacy policy. We have checked it.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- therapeutic drug monitoring
- pharmacy service
- hospital
- administration
- intravenous
- analytic sample preparation methods
- clinical laboratory techniques
Introduction
Amikacin is effective for a broad spectrum of bacterial infections in children and adults, especially severe gram-negative infections. Despite widespread bacterial resistance, amikacin remains one of the most frequently prescribed antibiotics.1 2 Amikacin is a hydrophilic compound, which is well distributed throughout the body after intravenous administration and mainly eliminated through glomerular filtration.3 The efficacy of amikacin exhibits a concentration-dependent pattern and the use of amikacin is limited by its ototoxicity, nephrotoxicity and other side effects. The therapeutic window for amikacin is narrow and the relationship between the dose and the measured plasma concentration is complicated.4 5 According to the US Food and Drug Administration’s (FDA’s) guideline and label information, amikacin’s peak concentration (Cmax) and trough concentration (Cmin) of normal adults should be less than 35 µg/mL and 5 µg/mL, respectively.6 The regimen for elderly, children, and patients with impaired renal function should be especially individualised. Consequently, therapeutic drug monitoring (TDM) is a crucial part of the service provided by clinical pharmacists for patients during treatment with amikacin. The effective pharmacodynamic parameter for amikacin is Cmax in plasma over minimal inhibitory concentration and Cmin is related to its toxicity.7 These parameters were recognised as the reference for amikacin efficacy and adverse reactions to serve the clinical needs.
The assay for plasma amikacin quantification by liquid chromatography-tandem mass spectrometry (LC-MS/MS) has been established for clinical use since 2018 and the amikacin samples are analysed within 1 day after acceptance. The amikacin results are provided as part of the TDM service by clinical pharmacists, which are interpreted and discussed in the clinical team for ongoing clinical management. According to the reference, clinical pharmacists have analysed and optimised the usage of amikacin by literature research, computer programs and questionnaires.8–10 However, few reports summarised the prescribing decisions before and after the assay for plasma amikacin concentrations and the possible relationships. In this study, we offered an LC-MS/MS plasma amikacin assay as a routine clinical pharmacy service. This research aimed to discuss the extent and reason for the use of plasma amikacin quantification and the subsequent prescribing decisions made by clinicians after the TDM results.
Methods
Chemicals
All the chemicals were of HPLC (high-performance liquid chromatography) grade. Amikacin and isepamicin were purchased from Dalian Melone Biotechnology Company (Dalian, China). Acetonitrile and methanol were obtained from Merck company (Germany). Formic acid was from CNW Technologies GmbH (Germany). Water was purified with a Milli-Q reagent water system from Millipore Corporation (USA).
Preparation
The stock solution of amikacin (1.0 mg/mL) and isepamicin (internal standard (IS) 1.0 mg/mL) was prepared in purified water. Serial dilutions for amikacin were made at concentrations of 1, 2, 5, 10, 25, 50, 100, 200, 500, 750, and 1000 µg/mL for calibration standards and 4, 40, and 400 µg/mL for quality control (QC) samples. The internal reference solution (IS) was prepared at concentrations of 50 µg/mL. The plasma samples of calibration standards and QC were prepared by spiking 90 µL of blank human plasma with the 10 µL prepared dilutions above. A 100 µL human plasma sample was transferred to a centrifuge tube with the addition of 10 µL IS solution (50 µg/mL) and 400 µL methanol plus 0.1% formic acid. The mixture was vortex-mixed for 1 min and then centrifuged at 13 000 rpm for 10 min. A 10 µl supernatant of the resulting mixture was injected into the LC-MS/MS system for analysis.
LC-MS/MS analysis
The assay was performed on the LC-20A HPLC system (Shimadzu, Japan) and the API 4000 triple quadruple mass spectrometer (Sciex Applied Biosystems, USA). Liquid chromatographic separation was achieved by the ZORBAX Aq column (150×4.6 mm, 5 µm) at 25℃ with a mobile phase composed of 0.1% formic acid in water (phase A) and acetonitrile (phase B) at a flow rate of 1 mL/min in a run time of 7 min. For determination, the analytes were ionised by an electrospray ionisation (ESI) source in positive ion mode and the analysis was carried out by a multiple reaction monitoring (MRM) mode with ion transitions 586.3→425.3 m/z for amikacin (collision energy of 25 eV, declustering potential of 91 eV, entrance potential of 9 eV, cell exit potential of 8 eV) and 570.3→411.3 m/z for IS isepamicin (collision energy of 24 eV, declustering potential of 79 eV, entrance potential of 11 eV, cell exit potential of 12 eV). The following settings were used: ion-spray voltage of 5.5 kV, ion source temperature of 550°C, gas 1 of 50 psi (pounds per square inch), gas 2 of 50 psi, curtain gas of 30 psi, and the collision gas setting of 6 psi.
Method validation
The study protocol was approved by the Human Research Ethics Committee of Shanghai General Hospital. All method validation steps were based on the FDA guidance for bioanalytical method validation. The specificity was examined by the chromatograms of a blank human plasma sample, a blank plasma sample plus amikacin and IS solution, and a patient plasma sample after amikacin administration. The calibration curves were generated with 1 /x2 weighted regression by plotting the peak area of amikacin to IS (y) versus nominal concentrations of amikacin (x). The accuracy (relative error, RE) and precision (relative standard deviation, RSD) of the intra- and inter-day were analysed by the QC plasma samples. Five replicates were analysed in each of the analytical runs. The recovery of amikacin was determined by the comparison of the peak area between plasma with normal procedures and plasma spiked with amikacin at the step just before centrifugation. Analogously, the matrix effect was determined by comparison of the concentration between plasma spiked with amikacin and purified water spiked with amikacin. The stability of amikacin was analysed in three experimental designs. The freeze and thaw stability was determined after three freeze and thaw cycles. The samples were frozen at −80°C and thawed at room temperature in each cycle. The post-preparative stability of amikacin was analysed by the processed samples during storage at 4°C after 48 hours. The concentration of plasma samples at room temperature after 12 hours was to verify the stability of blood samples under normal hospital processing procedure.
Data collection and statistical analysis
The laboratory of the clinical pharmacy department in Shanghai General Hospital provided the plasma amikacin concentration of LC-MS/MS analysis as part of the TDM service. The trough concentrations were sampled 0.5 hours before the drug administration, and the peak concentrations were sampled 0.5 hours after the drug administration. The amikacin samples were analysed as soon as possible after the arrival of the plasma samples and the results were extracted from 1 March 2018 to 31 May 2020. To compare the TDM service impact on clinical amikacin usage, we extracted the usage number of amikacin from 1 January 2016 to 31 May 2020. The electronic health and medical records of related patients were collected and examined. The basic medical data included age, sex, results of aetiological examination, and infection diagnosis. In addition, the amikacin-related data included amikacin dose, indication for checking concentration, trough and peak concentration, plasma creatinine concentrations before and after amikacin administration, and subsequent prescribing decisions after the LC-MS/MS results. Descriptive statistics were calculated and summarised. Statistical analysis was computed by SPSS Statistics 19.0 software and GraphPad Prism.
Results
LC-MS/MS method validation results
The specificity chromatograms for blank plasma, blank plasma spiked with amikacin and IS, and patient plasma sample spiked with IS are shown in figure 1. The chromatography showed excellent peak shape and symmetry, and the retention times of amikacin and IS were 2.93 and 2.92 min, respectively.
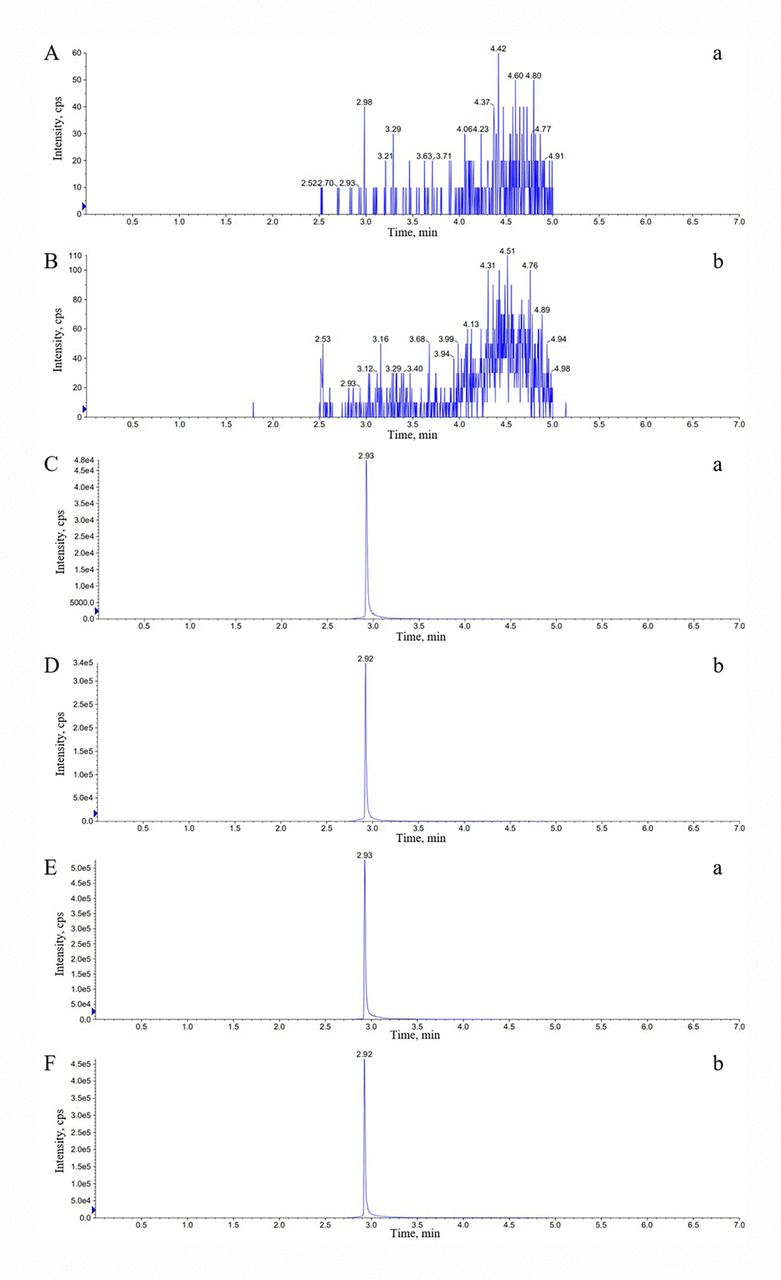
Typical chromatograms of amikacin and IS in human plasma. (A, B) Blank human plasma. (C, D) Blank human plasma spiked with amikacin and IS. (E, F) Patient plasma spiked with IS. (a) Amikacin. (b) IS. cps, cycles per second; IS, internal standard.
All performance indicating parameters are shown in table 1. The calibration curve for amikacin was constructed in the range of 0.1–100 µg/mL and the lowest limit of amikacin quantification was 0.1 µg/mL. The linearity of the calibration line was excellent and the equation was y=4.82×10−5x+5.97×10−3 (r2=0.9990). The intraday and inter-day variability for QC samples were within 11%. The extraction recovery and the matrix effect variability values of QC samples were <14%, which were within the acceptable range of FDA assay validations. Also, the QC samples showed no significant degradation for three freeze and thaw stability, post-preparative stability (48 hours at 4℃), and the stability for 12 hours at room temperature.
LC-MS/MS method for determining amikacin in human plasma
In conclusion, this method was validated and applied successfully to determine amikacin concentrations in patient plasma.
Characteristic analysis of amikacin samples and patients with amikacin concentration measurements
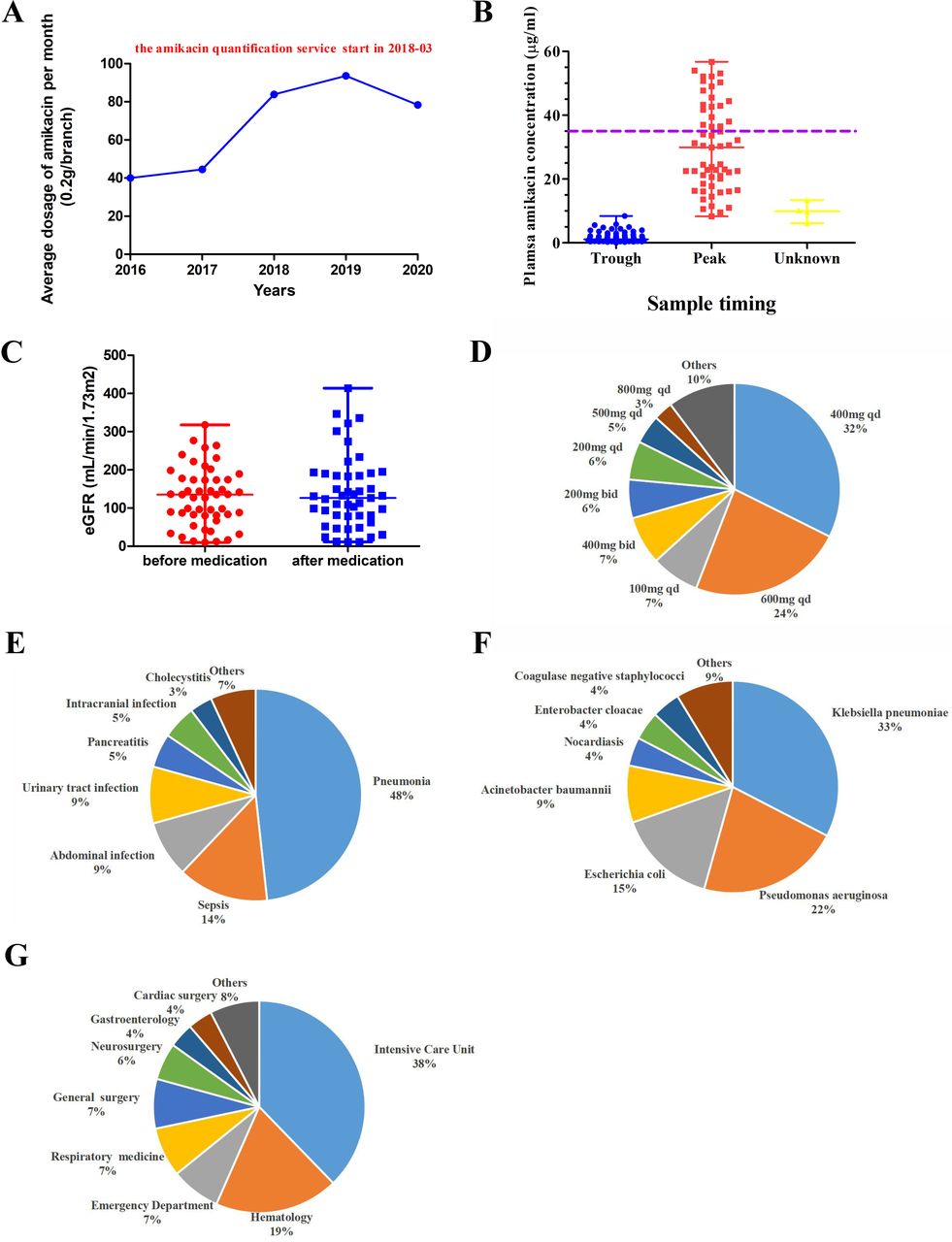
The demographic characteristics and clinical data of amikacin samples and patients with amikacin concentration measurements are summarised in table 2 and figure 2. In figure 2A, the usage of amikacin has significantly increased since 2018, mostly due to the amikacin quantification service started in March 2018. We included 121 amikacin plasma samples of 53 unique patients in this statistical analysis; 62/121 of these amikacin concentration samples were trough concentrations and the spread of measured sample concentrations is presented in figure 2B. Patients with peak concentrations >35 µg/mL should be monitored closely to avoid possible toxicity.

{kind=link}
{kind=link}
Characteristics of patients with amikacin concentration measurements. (A) The average monthly usage of amikacin. (B) The scatter plot of plasma amikacin concentrations (the violet line marks 35 µg/mL amikacin concentration, which was the update of the TDM crisis value in 2021). (C) The comparison of eGFR levels. (D) The distribution of amikacin doses. (E) The distribution of diagnoses. (F) The distribution of bacteria species. (G) The distribution of departments. eGFR, estimated glomerular filtration rate; qd, once daily; TDM, therapeutic drug monitoring.
Characteristics of amikacin samples and patients with amikacin concentration measurements
Regarding the patients, 73.6% were male, 43.4% were above 65 years old, and their clinical location at the time of amikacin sampling was inpatient mostly (96.7%, 117/121). Combination medication that may involve drug–drug interactions and exacerbate kidney function damage was the predominant indication for sample measurements (86.8%, 46/53). Patients above 65 years old or with impaired renal function were also important indications for sample measurement. The median estimated glomerular filtration rate (eGFR) after amikacin administration was slightly decreased compared with the median eGFR before amikacin administration in figure 2C. In the prescription of amikacin, 400 mg once daily and 600 mg once daily were the most frequent dosages and most of them were lower than the theoretical medication dosages in figure 2D.
In the statistics of infection diagnosis (figure 2E–F), 12 of 53 cases had multiple infections and pneumonia was the predominant infectious disease (48.3%, 28/58). In the 41 cases with complete aetiology examination, four patients were found with multiple pathogenic strains. Among them, Klebsiella pneumoniae (32.7%, 15/46) and Pseudomonas aeruginosa (21.7%, 10/46) were found most frequently. The intensive care unit (ICU) contributed to the largest number of patients in this analysis. We also summarised the therapy process of each patient to collect the prescribing decision after amikacin concentration measurement in figure 2G. These decisions were related to the amikacin assay results and clinical disease progression. Just under half (47.2%, 25/53) of these cases continued by changing to other antibacterial drugs, so the effective rate of amikacin administration was about 52.8% (28/53).
Discussion
Amikacin has been the most widely used semisynthetic aminoglycoside since the 1970s, when the problem of resistance caused by bacterial aminoglycoside modifying enzymes was overcome.2 For patients with serious infections caused by aerobic gram-negative bacteria, amikacin alone or in combination with other antibacterial drugs was commonly used.11 According to the 2018 national bacterial resistance surveillance report of the China Antimicrobial Resistance Surveillance System, gram-negative bacteria accounted for 70.6% of the bacteria included in the analysis. The top five isolates of gram-negative bacteria are Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Acinetobacter baumannii and Enterobacter cloacae. According to the aetiology examination, these were also the top five bacteria species detected of all patients receiving amikacin treatment in our study. The 2019 annual report of bacteria surveillance and drug resistance data analysis in Shanghai General Hospital pointed out that the bacterial resistance rates of amikacin were lower than most other antibacterial drugs. Apart from the amikacin resistance rate for A. baumannii (43%) which was higher than for the compound sulfamethoxazole (24.2%), the amikacin resistance rates for E. coli (1.9%), K. pneumoniae (3.6%), P. aeruginosa (5.9%), and E. cloacae (1.1%) were the lowest of all the tested antibacterial drugs. At present, amikacin is still one of the most effective antibacterial drugs for use in the treatment of the major gram-negative bacteria.
With the widespread use of amikacin, its related notable toxicity in the clinic setting became more apparent. Aminoglycosides appeared to cause nephrotoxicity in 25% of patients by accumulating in renal proximal tubular cells mostly. In addition, amikacin can generate free radicals within the inner ear and damage the sensory cells and neurons, resulting in permanent hearing loss.12 13 Nephrotoxicity, ototoxicity and neuromuscular toxicity caused by amikacin administration occurred in a dose-dependent and idiosyncratic manner, which was also related to old age, renal failure, therapy duration, higher trough levels, combination use of drugs with similar toxicity, and other possible factors.8 In the antibiotic stewardship programme of the 2016 Infectious Diseases Society of America guideline, the hospital implementation of pharmacokinetic monitoring and adjustment programmes for aminoglycosides was strongly recommended in order to reduce costs and decrease adverse effects.14 According to the international antimicrobial TDM report in 2020, routine TDM was recommended in critically ill patients accepted for aminoglycoside treatment, which had narrow therapeutic indices.15 China's National Medical Products Administration (NMPA) raised the announcement about the revision of the amikacin injection manual on 6 April 2021. It also mentioned that the blood concentration of amikacin should be monitored to ensure sufficient therapeutic concentrations and to avoid potential toxicity.
We started the project of plasma amikacin concentration analysis by LC-MS/MS in early 2018 and the assay was established and verified according to the related literature.16 17 Due to the clinical needs and the guideline’s strong recommendations, the amikacin concentration detection cases were increasing and the amikacin blood concentration monitoring projects were successfully carried out. However, the coronavirus pneumonia was severe at the end of 2019, which led to tightened hospital inpatient policies. Fewer patients were admitted, which indirectly led to a decline in the use of amikacin in 2020. According to our collected data, amikacin was the medication which was most frequently administered to inpatients in the ICU (38%), and these critically ill patients should be paid extra attention because of the influence of amikacin on the pharmacokinetic and pharmacodynamic parameters caused by the pathophysiological changes.18 19 To treat these systemic infections, the theoretical dosages of amikacin should be 15 mg/kg once daily or 7.5 mg/kg every 12 hours, but the actual dosages given in our hospital were lower than the calculated value in order to decrease the incidence of possible adverse events. In the past, little published evidence supported the optimal TDM targets for amikacin therapy; some studies targeted peak concentrations ranging from 15–40 µg/mL and trough concentrations lower than 10 µg/mL or 5 µg/mL.5 Thus, we classified most of the trough and peak plasma amikacin concentrations within the treatment window. According to the NMPA announcement in 2021, however, the peak concentration should be <35 µg/mL to avoid possible toxicity. Therefore, we revised the standard amikacin critical value reports. Clinical pharmacists would urge clinicians to adjust the prescribing decision when patients’ plasma amikacin concentrations were over 35 µg/mL.
Between 94–98.2% of amikacin is eliminated by the kidneys as unchanged drug, so patients should be given individualised doses based on their renal function. The level of eGFR that is estimated from plasma creatinine levels is one of the most commonly used metrics. Before amikacin therapy, 43.3% patients were found with below thresholds of eGFR concentrations, who should therefore be given reduced doses and their blood concentrations strictly monitored. The eGFR levels were elevated slowly from the start of amikacin therapy, consistent with former research, which were the clinical manifestations of nephrotoxicity.20 21 Apart from renal damage induced by diseases, the kidney function of the elderly and infants were also weaker than in healthy people. Among healthy adults, there was an obvious linear decline of eGFR at about 0.75 mL/min per year, and by the age of 90 years the average of eGFR was found to be reduced by 46% compared with younger adults.22 23 The elderly people (≥ 65 years old) in our study accounted for 43.4% of the total number of patients and the use of aminoglycosides should be monitored and carefully adjusted.24 Before the age of 2 years the kidneys have not yet fully developed, and the weakened renal function impacts not only on the clearance of drugs but also on the drugs’ absorption, distribution and metabolism.25 A limitation of our study is that no patients younger than 2 years were detected, in whom the aminoglycoside plasma concentration should be monitored, particularly in critical patients.26
In our study, the most common clinical disease diagnosis was serious pneumonia at 48%, and the largest proportion of sample measurement indications was the combination use of other ototoxic, nephrotoxic and neurotoxic medicines at 86.8%. On the one hand, most patients were diagnosed with severe infections or multiple organ infections, which required combination therapy with multiple antibiotics.27 On the other hand, some patients also had other diseases and needed to take medications such as diuretics and antidepressants. Intravenous administration was the most commonly used method for amikacin, but the limitation of this therapy was emphasised in the treatment of pulmonary infections of critically ill patients. According to the research, inhaled amikacin might overcome the problem of insufficient pulmonary distribution. Inhalation administration also reduced the toxicity and adverse effects caused by systemic exposure of antibiotics.28 29 According to our collected prescribing decisions regarding amikacin concentration, 47.2% of the patients changed to other antibacterial drugs, which might be due to the disappointing bactericidal efficacy, 22.6% of the patients got better and were discharged after amikacin administration, while the rest of the patients continued to use amikacin with or without dose adjustments. In the entire study, few severe adverse events have been reported. Besides, it is still too hard to quantify the impact of the amikacin concentration assay on prescribing decisions. However, both plasma concentration and renal function should be monitored in high-risk patients to avoid possible toxicity effects.30
Conclusions
Although it is one of the most popular antibiotics for gram-negative bacterial infections, amikacin has been limited in its clinical application because of its well-known toxicity and side effects. Thus, the plasma amikacin quantification assay should be established and carried out as part of the clinical pharmacist service in the hospital. The impact of amikacin concentration tests on its clinical application has still not been fully elucidated. This project should be continued to ensure the drug concentration of amikacin in patients remains within the treatment window to avoid possible side effects.
What this paper adds?
What is already known on this subject?
According to international antibiotic guidelines, the therapeutic drug monitoring practice programme for aminoglycosides was strongly recommended.
The efficacy of amikacin exhibits a concentration-dependent pattern and the use of amikacin is limited by its ototoxicity, nephrotoxicity and other side effects.
What this study adds?
We have successfully established an assay for plasma amikacin quantification by LC-MS/MS for clinical use since 2018, as part of the service provided by clinical pharmacists.
We collected and summarised the amikacin concentration results and the electronic health and medical records of related patients, and we found the assay results served as one of the references for amikacin prescribing decisions.
Data availability statement
The data were collected in the database of a third party which were not publicly available due to the patient privacy policy. We have checked it.
Ethics statements
Patient consent for publication
References
Footnotes
EAHP Statement 4: Clinical Pharmacy Services.
Contributors Conception and study design, Qin Li and Guorong Fan; new methods establishment, Lijie Xu and Juanni Hu; data analysis, Xuefang Cheng, Guanhua Zhu and Lijie Xu; writing-original draft preparation, Lijie Xu and Xuefang Cheng; writing-review and editing, Qin Li and Guorong Fan; funding acquisition, Qin Li and Guorong Fan. Guorong Fan is the guarantor.
Funding This work was supported by the Clinical Pharmacy Construction of Important Weak Disciplines of Shanghai Health and Family Planning Commission (No. 2016ZB0302).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.