Article Text

Abstract
Objectives: To clarify clinical manifestations, association with disease activity, and prognostic impact of thrombocytopenia using simple and reliable indices.
Methods: 632 patients were reviewed retrospectively. Fifty patients with thrombocytopenia were included as cases and matched with 100 control patients. Clinical manifestations at first thrombocytopenic episode were recorded. Classification criteria at diagnosis, basic immunological profiles, disease activity (ECLAM), and end organ damage (SLICC) were recorded.
Results: 29/50 (58%) had thrombocytopenia at diagnosis of lupus. Haemorrhagic manifestations were associated with the degree of thrombocytopenia (p<0.001). Anticardiolipin antibodies were not related to the degree of thrombocytopenia or the severity of haemorrhagic manifestations. Megakaryocytes were normal or increased in 26/28 (93%) bone marrow specimens, indicating peripheral platelet destruction. Patients with high disease activity were more thrombocytopenic than controls (OR = 2.61, 95% CI 1.13 to 5.96, p = 0.009). Patients with low C3 or CH50 were more likely to be thrombocytopenic (OR = 2.36, 95% CI 1.05 to 5.26, p = 0.029). Median SLICC for lupus patients with thrombocytopenia was 2 (range 0–11) compared with 1 (range 0–12) for controls (p<0.001). No deaths occurred during thrombocytopenic episodes.
Conclusions: Thrombocytopenia is not directly associated with end organ damage and mortality, but defines a subgroup of patients with higher morbidity and is thus a major complication of systemic lupus erythematosus, affecting overall prognosis.
- ACA, anticardiolipin antibodies
- CI, confidence interval
- ECLAM, European Consensus Lupus Activity Measurement
- ELISA, enzyme linked immunosorbent assay
- OR, odds ratio
- SLE, systemic lupus erythematosus
- SLICC, Systemic Lupus International Collaborating Clinics
- lupus
- thrombocytopenia
- manifestations
- activity
- prognosis
Statistics from Altmetric.com
- ACA, anticardiolipin antibodies
- CI, confidence interval
- ECLAM, European Consensus Lupus Activity Measurement
- ELISA, enzyme linked immunosorbent assay
- OR, odds ratio
- SLE, systemic lupus erythematosus
- SLICC, Systemic Lupus International Collaborating Clinics
Thrombocytopenia due to peripheral consumption of platelets is a common clinical manifestation in systemic lupus erythematosus (SLE), ranging from 7% to 30% in large reported series. Apart from diverse aetiologies in lupus thrombocytopenia, its clinical implications and prognostic impact still remain a matter of debate. Results of studies on the prognostic significance of thrombocytopenia in patients with SLE have been contradictory.1–3 In an endeavour to explain these disparate observations, a retrospective study was undertaken to analyse basic clinical and immunological characteristics, end organ damage, and disease activity in thrombocytopenic patients with SLE.
PATIENTS AND METHODS
All available 632 medical records of patients with SLE were reviewed to confirm the patients’ eligibility and gather demographic and clinical data from the time of diagnosis to enrolment. Case documentation, assessment of disease activity, damage events, and therapeutic interventions were made by the same group of rheumatologists throughout. Patients with SLE who had at least one episode of thrombocytopenia, defined as a platelet count of <100×109/l, were included in the study as cases, according to standard criteria.4,5 Each case was matched for age, sex, and disease duration with two patients with SLE who never developed thrombocytopenia.
Variables
Age, sex, clinical presentation, disease duration, disease activity, autoantibody profile, and organ damage were recorded. The criteria of the American College of Rheumatology for classification4 were obtained from all patients at the time of diagnosis. Disease activity was measured with the European Consensus Lupus Activity Measurement (ECLAM) score,6 calculated at the onset of thrombocytopenia in the case group. In this group, thrombocytopenia was not included in the ECLAM score in order to obtain a more accurate comparison of SLE activity between the two groups. In the control group the ECLAM score was obtained at the same interval from diagnosis (±1 month).
Organ damage was recorded at the end of follow up according to the Systemic Lupus International Collaborating Clinics (SLICC) Damage Index7 and was further classified into five broad categories as renal, neuropsychiatric, cardiovascular, pulmonary, and treatment related. The deceased cumulative damage was scored just before their death.
Antinuclear antibodies were determined by indirect immunofluorescence; anti-dsDNA by a standard enzyme linked immunosorbent assay (ELISA); anti-extractable nuclear antigens antibodies by counterimmunoelectrophoresis; serum C3 by nephelometry; CH50 by Autokit CH50, a commercial liposome immunoassay; and anticardiolipin antibodies (ACA) by a standard ELISA. Anti-dsDNA and serum C3 were measured frequently. ACA were tested at periods of disease activity. Complement levels and anti-dsDNA activity at thrombocytopenia in the case group and at matched disease duration for the control group were obtained for analysis.
Platelet number at the onset of thrombocytopenia, haemorrhagic manifestations, and number of relapses were also recorded for the case group. The presence of megakaryocytes was assessed by reviewing available bone marrow biopsy specimens at the onset of thrombocytopenia.
Various treatments were also recorded in both groups and broadly classified into low and high intensity regimens: the former comprised low dose corticosteroids with or without methotrexate or azathioprine and the latter, high dose corticosteroids with or without intravenous cyclophosphamide.
Statistical analysis
Continuous variables were compared using the Mann-Whitney U test. Categorical variables were compared using Pearson’s χ2 test, and odds ratios (ORs) with their corresponding 95% confidence intervals (CIs) were calculated. A multivariate logistic regression was used for adjusting parameter effects. The probabilities of damage-free and relapse-free intervals for different groups were determined by a Kaplan-Meier survival analysis, and curves were compared using the log rank test. Significance was defined as a p value <0.05. Data were analysed using the SPSS and Statistica software packages.
RESULTS
Case-control analysis
Fifty three (8.4%) patients with SLE and thrombocytopenia were found. Two patients with thrombocytopenia due to documented infection and one with methotrexate related bone marrow toxicity were excluded from the analysis. Fifty patients with SLE with thrombocytopenia and 100 without were finally included. Twenty eight had acute thrombocytopenia with platelets falling sharply to very low levels. Twenty two had had chronic, mild thrombocytopenia for months or years. Eight had thrombocytopenia preceding the diagnosis of SLE. Table 1 summarises individual demographic, clinical, and antibody profiles.
Demographic, clinical, and autoimmune profile among thrombocytopenic group and control group
The two groups did not differ significantly in their median ECLAM score (p = 0.12), but patients with high disease activity as denoted by an ECLAM ⩾4, were more likely to be thrombocytopenic than controls (OR = 2.61, 95% CI 1.13 to 5.96, p = 0.009). An analysis of complement activity showed similar results, and patients with low C3 or CH50 were more likely to be thrombocytopenic (OR = 2.36, 95% CI 1.05 to 5.26, p = 0.029), indicating a more active disease in thrombocytopenic patients. In logistic regression, the odds ratio of ECLAM ⩾4, adjusted for low complement, remained significant (OR = 2.46 (95% CI 1.05 to 5.75, p = 0.03)). No other differences in the basic clinical and autoimmune profiles were seen between the two groups. Thrombocytopenia itself, appears as a cause of high intensity immunosuppressive treatment in comparison with the control group (p = 0.009, table 1).
Haemorrhagic manifestations
Twenty nine (58%) of 50 patients had thrombocytopenia at diagnosis of lupus. These patients did not differ significantly in their clinical and serological characteristics from those developing thrombocytopenia thereafter. At presentation of thrombocytopenia, there was a strong association between the severity of haemorrhagic manifestations and the degree of thrombocytopenia (p<0.001) (table 2). The presence and isotype of ACA was unrelated to the severity of bleeding complications or the degree of thrombocytopenia.
Severity of haemorrhagic manifestations in patients with thrombocytopenia
Bone marrow findings
Twenty eight available bone marrow biopsy specimens during thrombocytopenic episodes were reviewed. Megakaryocytes were normal or increased in 26/28 (93%) specimens indicating peripheral platelet destruction. Two (7%) of 28 cases had a hypocellular and aplastic bone marrow, the former attributed to cytotoxic treatment and the latter to active disease.
Treatment and relapse of thrombocytopenia
Patients received high doses of corticosteroids intravenously or by mouth plus either pulse cyclophosphamide (17/53) or azathioprine (5/53) with or without intravenous globulin (12/53). Two of 53 patients were splenectomised. All patients finally achieved normal platelet counts.
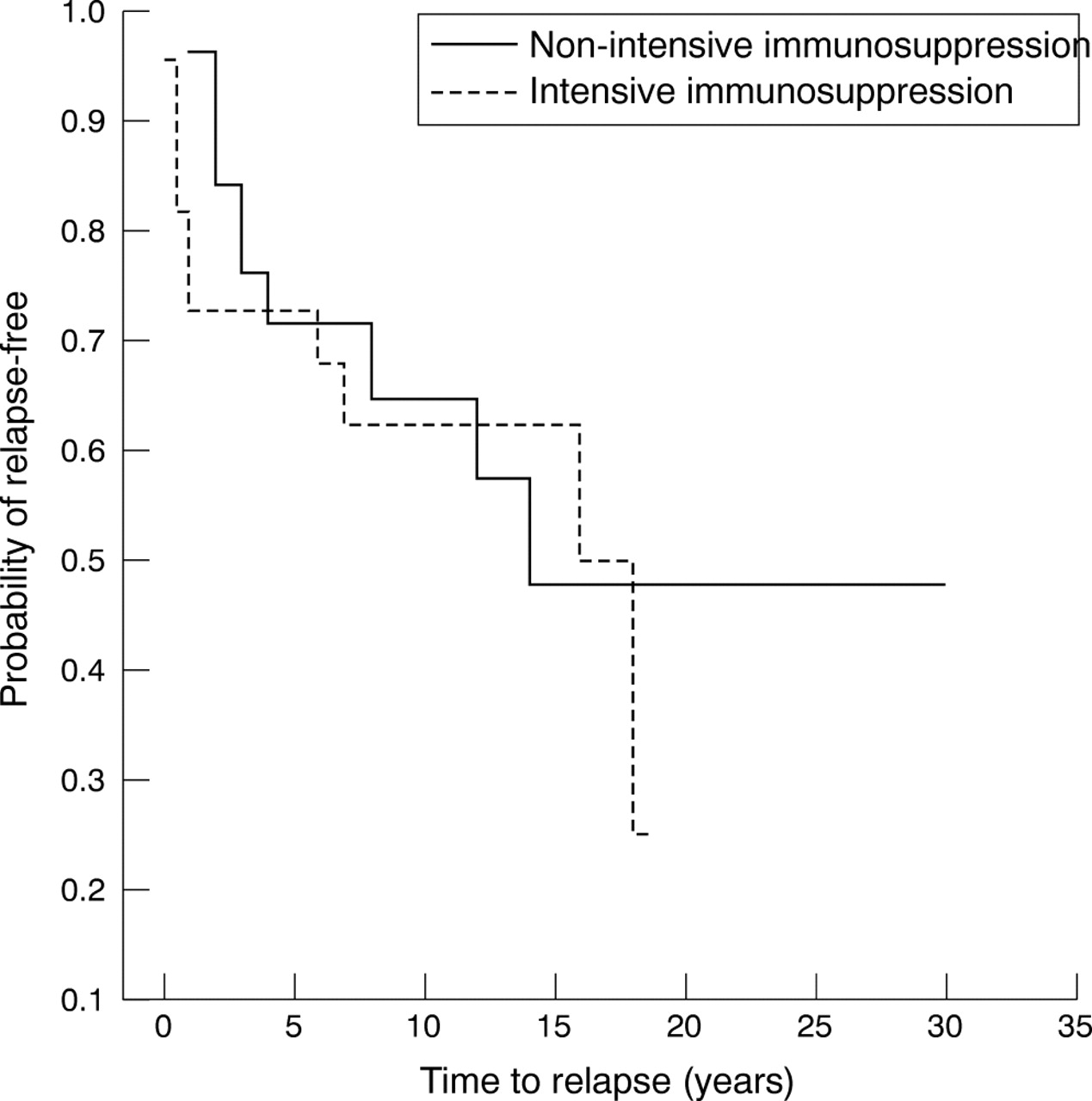
Twenty two (44%) of 50 patients had at least one relapse during the course of their disease, defined as a reduction in platelet count below the threshold of 100×109/l after achievement of a normal platelet count on at least two consecutive measurements. The probability of relapse-free intervals among thrombocytopenic subjects did not differ (p = 0.61) with treatment: low (n = 26) versus high intensity (n = 22) (fig 1).

Kaplan-Meier curves for patients with SLE and thrombocytopenia and with and without intensive immunosuppression (p = 0.61), showing the probability of a relapse-free interval.
ACA, severity of haemorrhagic manifestations, and high versus low ECLAM scores had no significant effect on the time to relapse (data not shown).
Overall morbidity
The two groups differed significantly in the number of end organ damage events, measured by the SLICC score at the end of follow up. Patients with thrombocytopenia had a median SLICC of 2 (0–11) in contrast with controls who had a median of 1 (0–12), reflecting a more aggressive course among thrombocytopenic subjects (p<0.001). The two groups did not differ significantly in their organ involvement and treatment related sequelae. A striking exception was the coexistence of renal disease and treatment related complications among thrombocytopenic subjects in contrast with controls (p<0.001) (table 3).
Cumulative organ damage at the end of follow up
There was no difference in the probability of a damage-free interval between cases and controls (fig 2). Separate analysis for each category of damage was also performed. Results were not significant (data not shown).

{kind=link}
{kind=link}
Kaplan-Meier curves for patients with SLE with thrombocytopenia (cases) and without thrombocytopenia (controls) (p = 0.14), showing the probability of a damage-free interval (time to first event). Median damage-free time for cases and controls were 10 and 14.5 years, respectively.
Deaths
Eight patients died during follow up, four in the thrombocytopenic group. No deaths were seen during thrombocytopenic episodes or associated with haemorrhagic complications. Pulmonary emboli, pulmonary infection, and central nervous system involvement (stroke, status epilepticus) were the causes of death (data not shown).
DISCUSSION
Miller et al suggested that thrombocytopenia did not determine patients’ subsequent course, but the coexistence of associated features such as glomerulonephritis and central nervous system involvement was a factor.8 Urowitz and Alger et al found no correlation with severe disease.9,10 In contrast, other authors identified thrombocytopenia as an important prognostic feature.11–13 Ward et al added thrombocytopenia to nephritis and seizures as features which adversely affect survival.1 Recently, Sultan et al associated thrombocytopenic manifestations with active disease in other organs, though none of these patients succumbed as a direct result of this complication.14
Differences of outcome in the abovementioned studies may be attributed, at least in part, to different treatment approaches, heterogeneity of the population such as ethnicity, and study design. As far as we know, this is the first matched case-control study providing a more accurate estimation of clinical characteristics, autoimmune profile, and prognosis in thrombocytopenic patients with lupus. At the onset of thrombocytopenia, patients have higher disease activity than their matched controls as measured using the ECLAM score. A score of four or higher is associated with a higher incidence of thrombocytopenia. If complement is used as a single estimate of disease activity, low values are also associated with thrombocytopenia.
In most patients thrombocytopenia follows a benign course and only a few patients had severe bleeding. Splenectomy was only performed on 2/14 (14%) occasions of severe (<20×109/l) thrombocytopenia, indicating a limited role for splenectomy. Although thrombocytopenia itself does not influence overall morbidity, cumulative organ damage, measured by the SLICC index, differs in the two groups. Patients with thrombocytopenia have a worse prognosis overall, as the SLICC index is a strong predictor of outcome and survival.15 Sites of organ involvement and treatment related complications do not differ between the groups. However, the coexistence of renal disease and treatment related complications is highly significant for the case group.
Our study has the limitations of a retrospective case-control study. However, all patients were attended by the same team of physicians at frequent intervals, medical records were routinely updated in detail, and possible sources of bias were limited. All patients were Greek in origin, so a separate analysis was unnecessary. The aforementioned conclusions, however, may not apply to other ethnic groups.
Our analysis indicates that lupus thrombocytopenia is a characteristic of active lupus. Although time to the first damage event does not differ between the two groups, thrombocytopenia emerges as a major indicator of cumulative morbidity among lupus patients. Thrombocytopenia should be considered as a reliable prognostic marker, identifying a subset of patients whose disease course is aggravated by end organ damage.
Acknowledgments
We are indebted to Professor HM Moutsopoulos, head of the department, for his inspiring recommendations and continuous support.
The study was supported by research funding from Genesis Pharma SA.