Article Text

Abstract
Introduction During the COVID-19 pandemic, measures have been put in place to adapt to patients’ needs during home quarantine, such as “telehealthcare”. With this service, hospital pharmacists develop a distinct role via the implementation of pharmacovigilance services and pharmaceutical care plans for patients with comorbidities, and for special populations as immunosuppressed patients.
Methods
Cross-sectional study involving hospital and community pharmacists actively practising during the COVID-19 pandemic. Patients who could not come to the hospital pharmacy department were provided with a delivery service to the community pharmacy of their choice.
Results A total of 1186 patients requested this service. Erythropoiesis-stimulating agents were the most in-demand medication, followed by rheumatoid arthritis and antiretroviral drugs. 125 patients responded to the telephone survey, most of whom stated that they would use the delivery service again, and expressed their desire to continue doing so.
Discussion Without a doubt, telepharmacy and medication delivery services have provided multiple benefits during home quarantine. The delivery service enabled us to provide drugs to patients in their immediate environment through a service that was free for both the patient and the hospital pharmacy service. However, at present, the available evidence of the impact of telepharmacy models is sparse.
Conclusions This medication delivery service has provided multiple benefits to patients during home quarantine. Although the users of this service seem to be satisfied with the current model, in the future, we should consider which patients would benefit most from this service and shape it to individual needs.
- hospital distribution systems
- medication systems
- hospital
- economics
- pharmaceutical
- pharmaceutical preparations
- pharmacy service
- hospital
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
- hospital distribution systems
- medication systems
- hospital
- economics
- pharmaceutical
- pharmaceutical preparations
- pharmacy service
- hospital
Introduction
In December 2019, the first case of coronavirus pneumonia (COVID-19) was detected in the city of Wuhan, Hubei province, China, which led to a nationwide epidemic. On 31 January 2020, the WHO declared the SARS-CoV-2 epidemic to be a “public health emergency of international concern”.1 On 11 March, COVID-19 became a pandemic and impacted more than 100 countries in the following weeks.2 SARS-CoV-2 is primarily transmitted human-to-human by respiratory droplets and close contact. It has an incubation period of 1–14 days before the onset of symptoms, however, the course of the infection can also be asymptomatic in a high percentage of patients. These COVID-19 characteristics underline the importance and urgency of preventing “community transmission” in overall pandemic control.3
During the COVID-19 pandemic, measures have been put in place to adapt to patients’ needs during home quarantine, such as “telehealthcare”. This term refers to the delivery of healthcare services through information and communication technologies (ICT), and also includes telepharmacy and telemedicine.4
Telepharmacy refers to the provision of pharmaceutical care through ICT to patients at a distance.5 It has many recognisable benefits such as easy patient access to healthcare services in remote and rural locations, savings on healthcare spending, patient satisfaction as a result of direct access to medication and information in rural areas, effective patient counselling, and a counterbalance to the scarcity of local pharmacist and pharmacy services. Telepharmacy is, undoubtedly, a great concept, but it is sometimes challenging to put into practice due to operational difficulties or lack of time, effort, and funds.6
A telepharmacy service enables hospital pharmacists to develop a distinct role via the implementation of pharmacovigilance services and pharmaceutical care plans for patients with comorbidities, and for special populations.7 8 It also allows the hospital pharmacist to perform a clinical-therapeutic assessment that is remote. This contributes to the fundamental objective of pharmacotherapeutic follow-up, namely guaranteeing the achievement of the pharmacotherapeutic objectives established for each type of patient.5 9
On 14 March 2020, the Spanish government declared a state of alarm to deal with the spread of COVID-19. Medication dispensing protocols were immediately established to deliver drugs to patients who could not come in person to the hospital pharmacy department.10 These measures were designed to benefit citizens unable to count on the support of others in their environment, those who could not journey from home due to mobility problems, who suffered acute illness or complex chronic processes that placed them in the highest risk categories for COVID-19 infection, those who, due to age or physical fragility, were more vulnerable to contagion, as well as those confined to home quarantine due to coronavirus.
The main objective of this study was to design a model that would facilitate access to hospital medication during home quarantine due to COVID-19, and ensure patient satisfaction with this process.
Methods
This was a cross-sectional study involving hospital and community pharmacists actively practising during the COVID-19 pandemic. The study was undertaken during the period of 28 March – 20 June 2020, a few days after the Spanish government’s declared state of alarm.
The study consisted of providing patients who could not come to the hospital pharmacy department with a delivery service to the community pharmacy of their choice.
Growth hormones, narcotics, and medication that required freezing for storage were excluded from the delivery service.
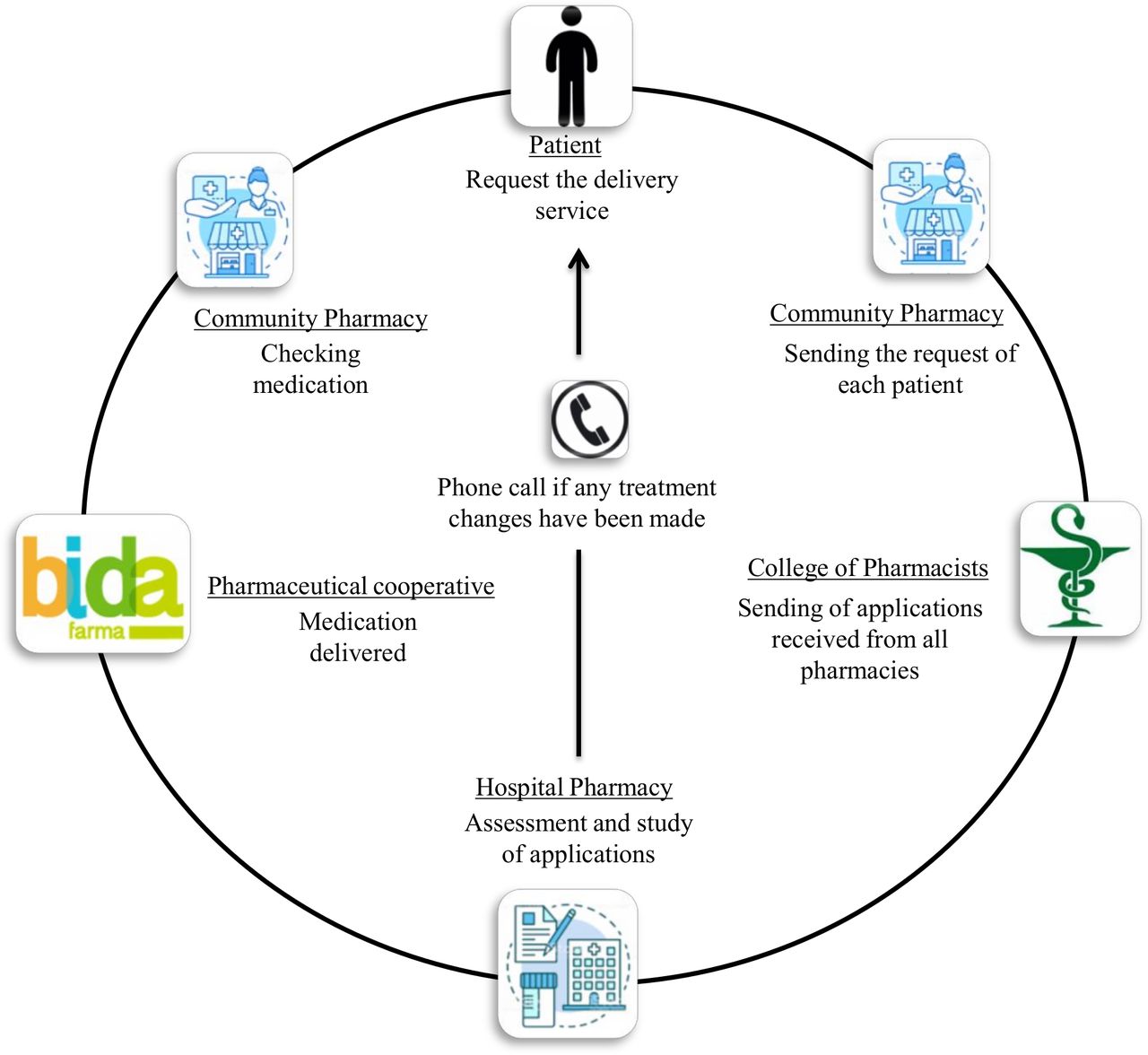
In order to establish this service, a detailed circuit was designed (figure 1). First, the patient voluntarily requested to be part of the delivery service, presenting a medical report to the community pharmacist and at the end of each day (Monday to Friday) the College of Pharmacists would collect the requests from all the community pharmacies and email them to the hospital pharmacy department. Later, the hospital pharmacist reviewed the patient’s electronic medical record, checking that the medication requested was appropriate, modifying it if deemed necessary (change of drug, dose, and so on). If there was a change in the patient’s treatment, usually through a telemedicine procedure, this was communicated to the patient by telephone. The medication was then packaged individually per patient in a black sealed bag with identifying labels of destination community pharmacies. The logistics service to deliver the medication from the hospital to the community pharmacy was established through a pharmaceutical cooperative, at no additional cost either to the patient or to the pharmacy department during the pandemic period. A traceable circuit was put in place since the label’s barcode linked the medication to the community pharmacy as the final destination. Finally, the community pharmacist who received the package checked the medication and, with the patient, reviewed and reinforced the information on the treatment. Before taking delivery of the medication, the patient signed a receipt certifying that they had taken possession of the medication. The process is, according to the Spanish personal data protection law “Ley Orgánica 3/2018, de 5 de Diciembre, de Protección de datos personales y garantía de los derechos digitales”, considering that, the contents of the bag (medication and patient identification) could only be seen by the community pharmacist.
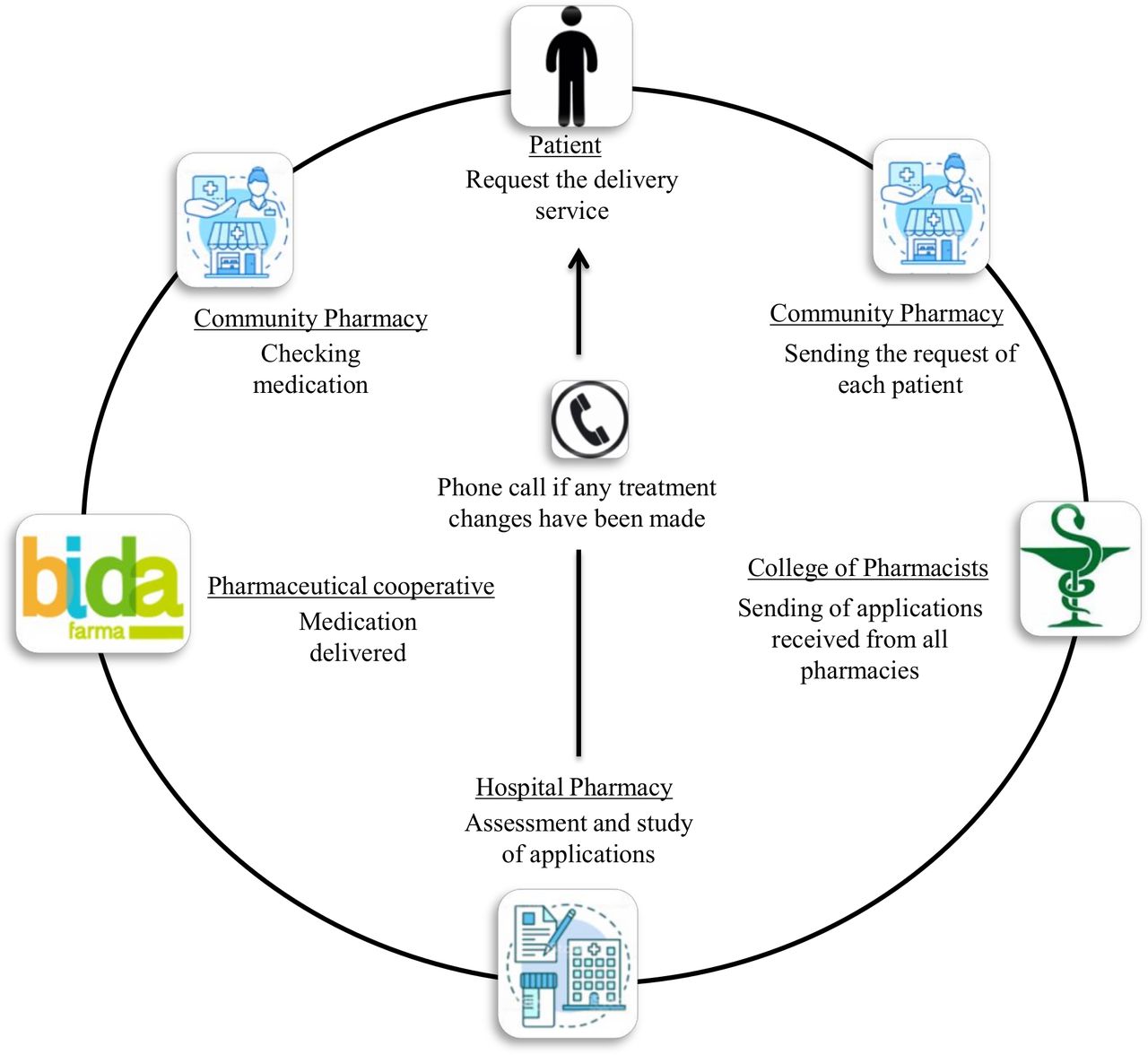
Circuit delivery service.
To measure user satisfaction with the model design, a telephone survey was performed to determine the degree of patient satisfaction with this service. The following assumptions were considered: an accuracy of 5%, a confidence level of 95%, and a response rate of 90%. The final sample size was 125 patients. All patients were eligible for random selection, and all agreed to participate. The survey included dichotomous qualitative variables (Scale: Yes/No) and a final question as a discrete quantitative variable (Scale: 1–10) that assessed the patient’s global satisfaction. Quantitative variables were given as mean and SD or as median and IQR in case of a skewed distribution. Qualitative variables were given as percentages (%). Statistical significance was set at less than 0.05. Data were analysed using IBM SPSS Statistics v 19.0.
Results
The participants in this project were the pharmacy department of the Juan Ramón Jiménez University Hospital, Huelva, Spain, community pharmacies in the province of Huelva (n=251), and a pharmaceutical cooperative as logistics service provider.
During the state of alarm, 1186 patients requested this service, which amounted to 1685 dispensations of medicine, since there were patients who requested this service on more than one occasion. Figure 2 shows how the number of patients who requested the service developed during the state of alarm.
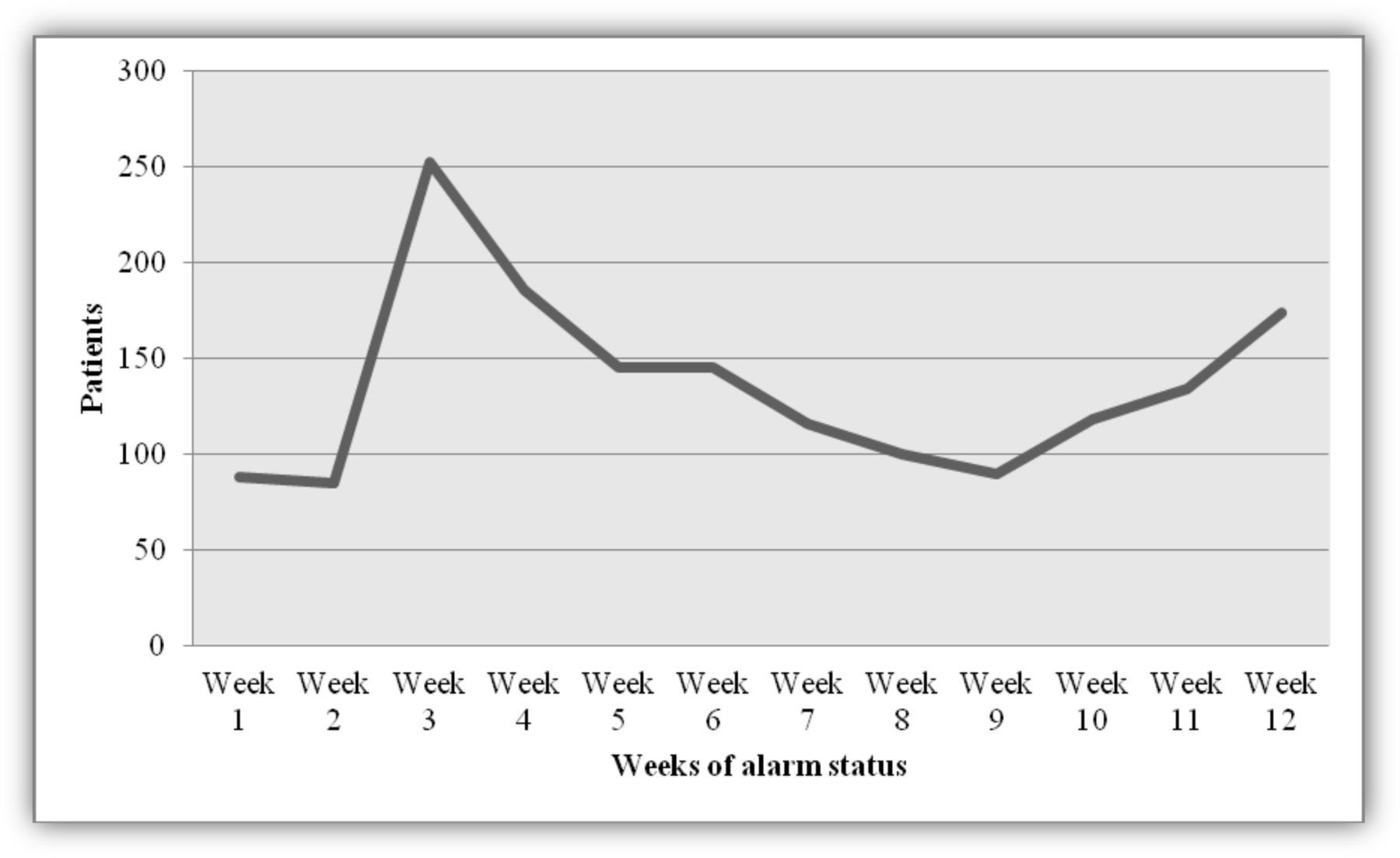
Evolution of the number of patients who required the home delivery service during the state of alarm.
Table 1 shows the profile of the medication requested by the patients. Erythropoiesis-stimulating agents were the most in-demand medication, followed by rheumatoid arthritis and antiretroviral drugs.
Profile of the medication requested by the patients
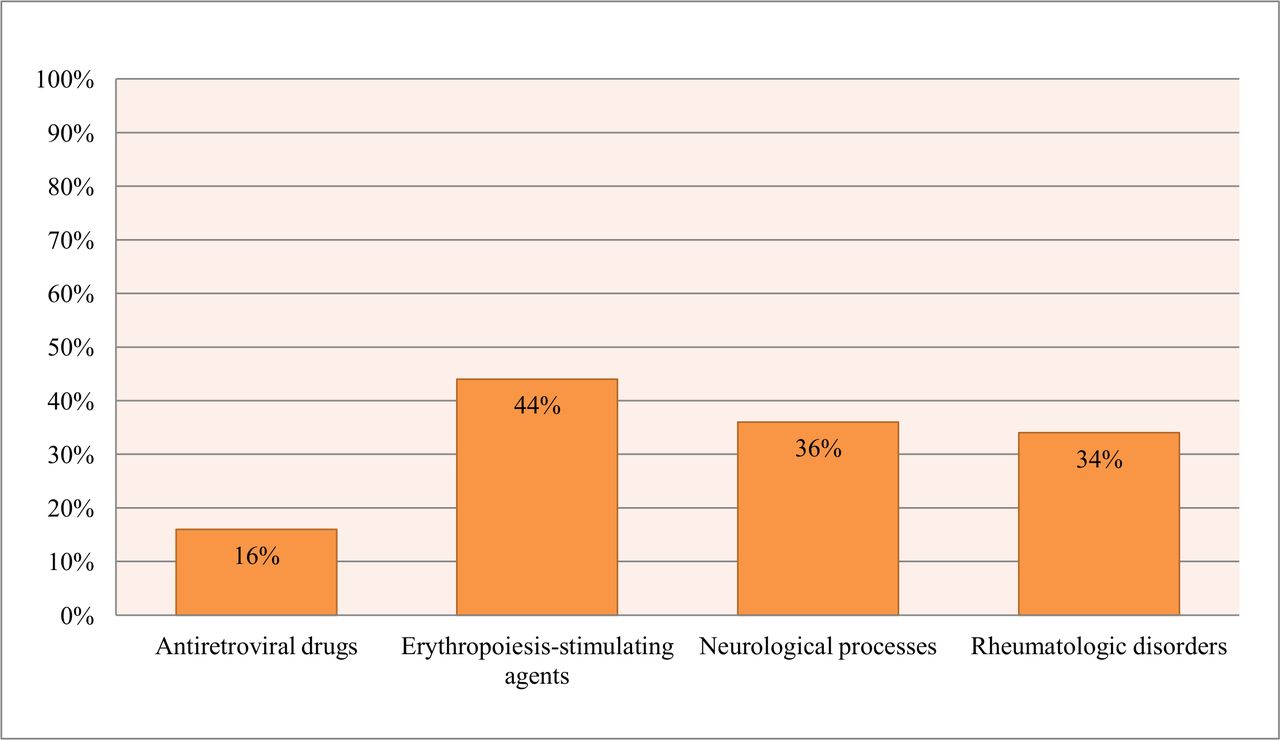
During 2019, the outpatient area of Juan Ramón Jiménez Hospital dispensed medication to 5939 patients. Based on this figure (figure 3), the service developed in this project covered 20% of the patients. Figure 3 shows the main types of patients who used the home delivery service with respect to the total of outpatients who received medication in 2019.
{kind=link}
{kind=link}
{kind=link}
Main types of patients included in the home delivery service compared with the total of outpatients in 2019.
There were incidents during the delivery service (n=10), which were: no drug delivery (30%), dosing error (20%), wrong drug (20%), unnecessary drug (10%), wrong formulation (10%), and wrong patient (10%). All these incidents were resolved satisfactorily.
Regarding patient satisfaction, 125 (10.5%) patients responded to the telephone survey, 67 (54.5%) being women. Of those surveyed, and according to the location of the community pharmacies where they collected the medication, 55 (44.7%) resided in the provincial capital (Huelva) and 68 (55.3%) in towns in the province. Table 2 shows that most of the patients surveyed stated that they would use the delivery service again, and expressed their desire to continue doing so. Mean global satisfaction was 9.83±0.568 points.
Telephone survey to determine the degree of patients' satisfaction with the delivery service
Discussion
To the authors' knowledge, this is the first study that reports the results of a telephone survey on the delivery of medication during the COVID-19 pandemic. The results obtained indicate that the pilot service would have a high probability of success since patient satisfaction with the model is good.
The pandemic has led to the acceleration of the development of circuits and strategies which, under normal conditions, would have taken months to set up.11
Without a doubt, telepharmacy and medication delivery services have provided multiple benefits during home quarantine. However, we must bear in mind that not all patients have the same needs. Further action is needed to identify which groups of patients require more intensive pharmaceutical care and, therefore, who could benefit most from telepharmacy, and not only the delivery service. The goal is to continue to provide high quality care.
On the other hand, regulations need to be established to organise all these circuits beyond the rules imposed because of COVID-19. The drafting and implementation of a uniform, comprehensive law on telepharmacy law still needs to be addressed.12 13
In our case, the delivery service enabled us to provide drugs to patients in their immediate environment through a service that was free for both the patient and the hospital pharmacy service, and which reached 20% of our outpatient population.
According to the literature, the combination of telepharmacy and home delivery has now become the most widely used model.14–17 Peterson et al14 describe a model where the pharmacist holds a video consultation with the patient to ensure that they understand why the medication is being prescribed and how to administer it correctly. Leon et al15 conducted appointments via videoconferencing and virtual consultations that covered compliance, adverse events, or interactions, after which medication was delivered to the patient by courier. In a few cases, patients were selected for telepharmacy. León et al15 selected stable chronic human immunodeficiency virus-infected patients, and Young et al16 selected from a rural population of patients who suffered from asthma. In most cases, the cost of the telepharmacy and home delivery services was paid for by the hospital pharmacy department, not by the patient.14–18
At present, the available evidence of the impact of telepharmacy models is sparse. Despite the fact that there are no studies that focus on the community pharmacy matched to a medication delivery service, our experience has been very positive in that it has enabled us to bring hospital medication closer to the patients in a difficult and disruptive time for society, still within a healthcare environment, and with no extra cost to the public healthcare system.
The delivery model that could well outlast the pandemic is one that is viewed positively by patients and covers all their needs. This model also identifies which patients could benefit from this new pharmaceutical model.
Finally, the implementation of this novel home delivery service during the pandemic enabled us to provide coverage across the entire province of Huelva, since it encompassed all community pharmacies in the area, and it allowed us to develop logistics specialised in medicine, in particular a medication delivery service that also involves a healthcare professional (the pharmacist) who can reinforce the necessary information with the patient on delivery, and a cost-free model for all those involved during the state of alarm.
Conclusions
This medication delivery service has provided multiple benefits to patients during home quarantine. Although the users of this service seem to be satisfied with the current model, in the future, we should consider which patients would benefit most from this service and shape it to individual needs. As pharmacists, we must add value by focusing on the patient, not on the drug or disease, identifying the needs of each patient in detail.
What this paper adds
What is already known on this subject
With the delivery of healthcare services through ICT, the patient has access to healthcare services in remote and rural locations, saving on healthcare spending.
What this study adds
A delivery model that could well outlast the pandemic is one that is viewed positively by patients and covers all their needs.
Coordinated action with community pharmacies and a pharmaceutical cooperative was essential for implementation of this novel home delivery service during the pandemic.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
We wish to thank the College of Pharmacists, all the community pharmacies in the province of Huelva, and the pharmaceutical cooperative Bidafarma, all of whom have collaborated selflessly in this project during the COVID-19 pandemic.
Footnotes
EAHP Statement 5: Patient Safety and Quality Assurance.
Twitter @awina87
Contributors We can confirm that everyone listed met the ICMJE criteria for authorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.