Article Text

Abstract
Objective The aim of this study is to describe and categorise pharmacist interventions (PIs) in a central hospital and report acceptance rates by physicians.
Methods A retrospective study was carried out in a 350-bed central hospital between January and June 2013. Eleven pharmacists screened the pharmacotherapy charts for drug-related problems leading to PIs. The recommendations resulting from this analysis were entered in the electronic prescribing system. All the PIs registered on the electronic medical record system during the study period were eligible for inclusion. Interventions were quantified and characterised. Computer records were consulted to assess acceptance rate by physicians.
Results A total of 1249 PIs were made by 11 pharmacists, and covered 147 drugs, with the most common being antibacterial (25%) and for the central nervous system (24%) and cardiovascular system (18%). Of the 1249 PIs, 18% concerned acetaminophen, 13% enoxaparin and 10% amoxicillin/clavulanic acid. The PIs were classified into three main categories: drug, dosage and administration related. When we analysed the most relevant PI type (n>20), the highest acceptance rate was for dosage adjustment according to therapeutic indication (58.1%) and renal function (57.4%). The global rate of acceptance was 53%.
Conclusions Pharmacists’ recommendations entered in the electronic prescribing system with a short explanation, as well as the pharmacotherapy recommendation, are immediately available to the doctor; however, the relatively low acceptance rate suggests that a further study also evaluating verbal interventions is needed, since the most urgent recommendations are made verbally, and this would likely increase the acceptance rate.
- CLINICAL PHARMACY
- EPIDEMIOLOGY
- MEDICAL ERRORS
- PHARMACOTHERAPY
- INSTITUTIONAL MEDICATION SURVEILLANCE
Statistics from Altmetric.com
Introduction
Drug prescription is the most common medical intervention in the provision of healthcare. Clinical pharmacy is defined as the provision of patient-oriented pharmaceutical care, with the goals of maximising drug efficacy and minimising drug harm by preventing drug-related problems.1 Clinical pharmacy has been practised in most European countries for several years.2 The clinical and economic impact of clinical pharmacy has been addressed in many studies, and the value of clinical pharmacy has been shown by the improvement in both clinical and economic outcomes.3–8 Medicines optimisation is about ensuring that the right patient receives the right medicine at the right time. By focusing on patients and their experiences, the goal is to help patients improve their outcomes, take their medicines correctly, avoid taking unnecessary medicines, reduce wastage of medicines and improve medicines safety. Ultimately medicines optimisation can help encourage patients to take ownership of their treatment.9
In hospitals, clinical pharmacists are working on the wards and are part of the multidisciplinary team. They analyse patients’ pharmacotherapy profiles in relation to their medical and laboratory data. When appropriate, they recommend drug therapy changes to physicians and nurses, and answer questions about drugs.2 Pharmacists routinely make clinical interventions in order to improve the health outcomes of patients.10 Most interventions by pharmacists consist of medication profile review to address potential drug-related problems. The medication profile review includes consideration of the medication history, identification of medication problems, and recommending a plan of action.11 Several studies described the interventions of pharmacists in adjusting and optimising drug therapy, making therapeutic recommendations and interacting with physicians, performing continuous laboratory monitoring of specific parameters, and evaluating medication appropriateness. The participation of pharmacists in medical rounds was also reported in some studies. Pharmacists’ interventions may have a positive impact on the outcomes for a specific group of patients, namely those with chronic kidney disease.12
Medication review can be defined as ‘a structured, critical examination of a patient's medicines with the objective of reaching an agreement with the patient about treatment, optimising the impact of medicines, minimising the number of medication related problems and reducing waste’. This concept can also be applied to hospitalised patients where the doctor is the person whose agreement must be obtained. Medication review should check that the medication prescribed is appropriate for the patient's needs, is effective for the particular patient, is a cost-effective choice, and any required monitoring has been done or has been arranged. Pharmacists performing the review must consider several factors, namely drug interactions, side effects, over-the-counter and complementary medicines, and unmet need. According to some authors, dose optimisation does not count as a full clinical medication review, but may be useful as part of the medication review process.13 Medication review is increasingly recognised as a cornerstone of medicines management, preventing unnecessary ill health and avoiding waste. In 2008, the National Prescribing Centre published A Guide to Medication Review which described three ‘types’ of review, with the third type being clinical medication review, which addresses issues related to the patient's use of medicines in the context of their clinical condition.14
Our study examined pharmacist interventions (PIs) made during the validation process of computerised prescription, taking the patient’s clinical condition into consideration, in order to improve the health outcomes of patients hospitalised in our hospital centre. The objective of the study is to describe medication interventions, categorise intervention types and report acceptance rate by prescribers.
Methods
A retrospective study was carried out in S. Francisco Xavier hospital (350 available beds, mainly acute), which is part of the West Lisbon Hospital Centre, between January and June 2013. The hospital centre includes three hospitals, each dedicated to different but complementary specialties. Emergency, oncology, haematology, obstetrics, paediatrics, orthopaedics, surgery and internal medicine are located in S. Francisco Xavier hospital. The hospital centre has one pharmaceutical service with a satellite pharmacy in each hospital. Practices and indicators assessed in each satellite pharmacy are standardised.
Eleven pharmacists screened the pharmacotherapy charts for drug-related problems leading to PIs. Pharmaceutical validation was performed on computerised prescriptions, according to a standardised method and after consulting medical and nursing files and laboratory values. At the time of the study, medical files, laboratory values and medication administration records were available mainly in the electronic patient file. Paper records were consulted on the ward. PIs were recorded in the electronic prescribing system, and were immediately available to the physician. Each drug-related problem was specified, with a short explanation, as well as the pharmacotherapy recommendation. All the PIs registered on the electronic medical record system during the study period were eligible for inclusion. Interventions were quantified and characterised. Acceptance by physicians was also evaluated by a pharmacist, who classified the interventions as ‘accepted’ or ‘not accepted’. Medical acceptance was defined as changing the prescription within 48 h after a PI.
Results
During the study period (January–June 2013), 11 pharmacists screened the pharmacotherapy charts of 3604 patients for drug-related problems, leading to 1249 PIs for 147 drugs. These were mainly antibacterial, central nervous system (CNS) and cardiovascular system drugs, with acetaminophen, enoxaparin and amoxicillin/clavulanic acid most commonly involved (tables 1 and 2).
Distribution of drugs involved in pharmacist interventions
Drugs with most interventions
The pharmacists screened pharmacotherapy charts for the following underlying drug-related problems: dosage adjustment (renal function, obesity, paediatric, pharmaceutical form and according to indication), drug related (justification request, contraindication, unnecessary use, untreated/reconciliation, drug interaction and adverse drug reaction) and administration related (route, timing and incompatibility). The most frequent PIs were dose related and the majority of these were for dose adjustment because of patient renal function (table 3)
Distribution of interventions by type
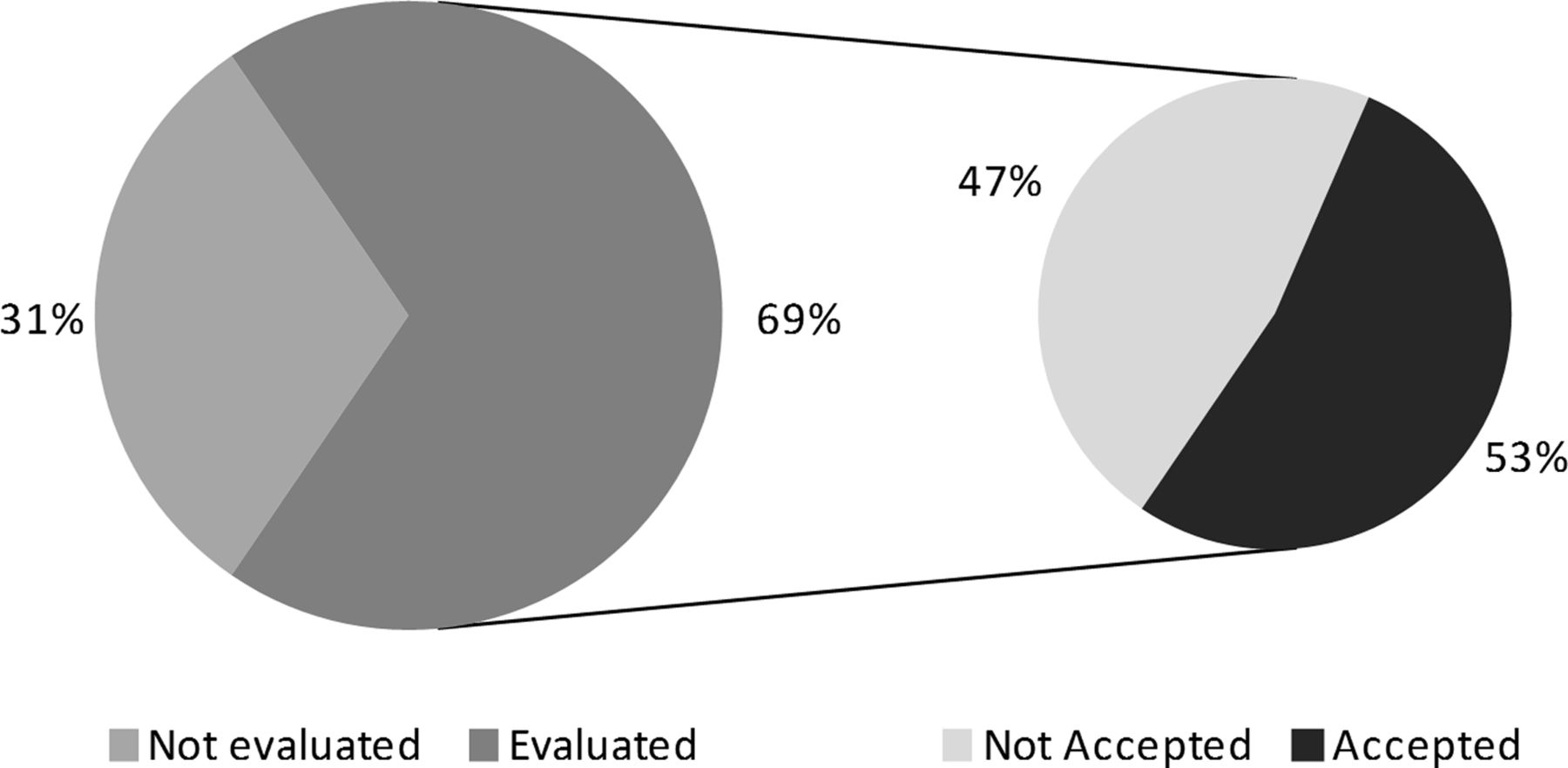
Acceptance rate was assessed in 856 (68.5%) PIs. The acceptance rate differed according to the type of intervention. The most frequently accepted type of PI was dose related as shown in table 4. Of the 856 (69%) PIs evaluated, 450 (53%) were accepted as summarised in figure 1.
Acceptance rate of pharmacist interventions

{kind=link}
Evaluated pharmacist interventions and acceptance rate.
Discussion
Collaboration between physicians, nurses and pharmacists is normal in our hospital centre. Pharmacists are fully integrated into the multidisciplinary team, so medication review is part of pharmacist daily practice. During the study period, all patient prescriptions (n=3604) were reviewed by pharmacists. Interventions were made for 147 drugs, mainly antibacterial, CNS and cardiovascular system drugs as found in other studies.(Survey, Candice, Annemie, Bedouch 2008) The majority of interventions involved antibacterial drugs (n=543; 43.5%). These data are in accordance with the results from the Institute for Safe Medication Practice Survey where the most common intervention was for this therapeutic group.15 The majority of the PIs concerned acetaminophen (n=226), probably because during the study period pharmacists were promoting a switch from intravenous to oral administration, where possible, as the result of a previously identified drug-related problem. When we analysed the PIs by type, the most frequent reason for the interventions involved dose (n=548; 43.9%) as seen in other studies. (Nick; Boden; Annemie; Hawkey)
The acceptance rates for recommendations made by clinical pharmacists to physicians were generally high, varying from 39% to 100%. Only 2% of the interventions concerned drug interactions, due to the existence of automatic alerts on the electronic prescription system that were implemented during the study period. Five of the drug-interaction interventions identified and evaluated for acceptance were major and four were moderate. Only one of the major interactions was not accepted, and concerned the interaction between haloperidol and trazodone, which has a fair reliability rating.16 The low number of interventions related to adverse drug reactions does not allow further analysis. The low acceptance rate of the interventions related to contraindications is due to the fact that metformin is contraindicated in patients with creatinine clearance less than 60 mL/min as documented in the summary of product characteristics. However, NICE (National Institute for Health and Care Excellence) and HAS (Haute Autorité de Santé) advise against the use of metformin only for values less than 30 mL/min. We were not able to evaluate the acceptance rate for 393 interventions due to patient discharge or transfer between wards before the physician could see the recommendation.
The patient characteristics and the types of drugs prescribed are probably comparable to those in other hospitals; however, prescribing rules and the working methods of physicians and pharmacists may differ between institutions. The detection of drug-related problems and the recommendations provided could strongly depend on the experience of the clinical pharmacist involved. The hospital pharmacists are similar in terms of age and professional experience (all with more than 5 years of experience), so interventions were not stratified on pharmacist. No clinical endpoints were taken into consideration (eg, hospital readmissions, mortality or quality of life). Also, the lack of a control group of patients not undergoing the intervention can be considered a weakness of the study design. Moreover, the aim of this study was not to assess the impact of the clinical pharmacist on clinical outcomes.
The information technology used in our hospital enabled recommendations to be made in the electronic prescribing system and provided immediately to the doctor. Each drug-related problem was specified, with a short explanation, and presented together with a pharmacotherapy recommendation. However, when we analysed acceptance rates by intervention type, we found that it was 57.5% for dosage, 46.2% for drug and 50.0% for administration. These data were somewhat lower than reported in other studies.3 ,17–22 This could probably be explained by the fact that the pharmacist was not present when the recommendations were considered by the treating physician, precluding further discussion at that time.
It should noted that interventions made during ward rounds were not considered in this study since they are not entered in the prescription system. For further evaluation it would probably be interesting to evaluate the acceptance rate by ward speciality or by junior versus senior doctors. The role of the clinical pharmacist might be to detect the over- and underuse of drugs, and to discuss therapeutic goals and drug use with physicians. Pharmacist's recommendations entered in the electronic prescribing system with a short explanation, as well as the pharmacotherapy recommendation, are available immediately to the doctor; however, the relatively low acceptance rates suggest that further study including verbal interventions is needed, since the most urgent recommendations are made verbally, and this would likely increase the acceptance rate.
Conclusion
In conclusion, pharmacists’ interventions can contribute to improved drug therapy and lead to increased medication safety.
Key messages
What is already known on this subject
-
The clinical and economic impact of clinical pharmacy has been demonstrated by improved clinical and economic outcomes.
-
Clinical pharmacists are working on the wards in hospitals and are part of the multidisciplinary team.
What this study adds
-
Pharmacists’ recommendations entered in the electronic prescribing system are immediately available to the doctor.
-
The relatively low acceptance rate of pharmacists’ electronic recommendations suggests that a pharmacist presence on the ward is essential to the practice of clinical pharmacy.
References
Footnotes
-
Contributors All authors made pharmacist interventions during the study period, and all contributed to the study design, and analysis and processing of data. FF, EV, CL and RB drafted the article.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.