Article Text

Abstract
Purpose Birmingham Children's Hospital in the UK provides family centred care for post-transplant medication (PTM) management. Nevertheless, PTM is often considered a burden for patients, and can be difficult to manage. This study was designed to identify the main medication issues encountered by children and their parents in order to find suitable means to improve their care management.
Method Anonymised multifactorial, cross-sectional, single-site survey. Parents of children transplanted from January 2011 were recruited following two strategies: (1) self-completion of questionnaire at the outpatient department over a period of 4 weeks during May 2013, (2) telephone completion by random selection of 30 parents. Results were analysed using MS Excel 2010.
Results 37 parents were recruited. Medication supply problems concerned 12 (32.4%) parents. 30 (81.1%) parents declared having almost run out of medicines, but no children missed an immunosuppressant dose. 9 (24.3%) parents experienced medication-administration problems, and 14 (37.8%) blood test issues. 14 (37.8%) parents felt they had an inadequate knowledge of side effects. However, 30 (81.1%) parents thought that their training was excellent or very good, and 36 (97.5%) that the written information provided was comprehensible and accurate. Among proposed improvements, parents’ preferences were for an online learning tool (OLT), an explanatory comic book (CB) for children and pharmaceutical consultations (PC).
Conclusions To our knowledge, this study is the most comprehensive published audit concerning the care process of PTM. Although parents seemed particularly satisfied by the current training and written information, many experienced issues linked to PTM management. Based on parents’ preferences, a working party is currently considering service development options (OLT, CB, PC).
- Liver Transplantation
- Paediatric
- Family-Centred Care
- Patient's Perpective
- Medication Issue
Statistics from Altmetric.com
Introduction
Patients undergoing renal, liver and other transplants require careful management and close cooperation between healthcare professionals before and after the transplant.1 ,2 Immunosuppressant pharmacotherapy is a critical aspect of post-transplant patients’ care. Patients must take immunosuppressants for the remainder of their lives to prevent episodes of graft rejections.3 Although transplantation is perceived as a new chance of life, the need to take these post-transplant medications (PTM) are often considered as a new challenge. Non-adherence to PTM is an important issue for paediatric patients who had transplants. In a recent meta-analysis, the rate of non-adherence was reported to be from 3% to 71%, with the worst rate in adolescent patients who had transplants.4 Serious consequences are associated with non-adherence to PTM. These include: increased risk of graft rejection and post-transplant mortality, poor health-related quality of life and increased healthcare costs.5–7
In paediatric settings, any agreement regarding medical care will often rely on parents’ understanding and cooperation. The dynamics of interaction between paediatric patients and healthcare professionals are complex given that parents usually take the lead as an intermediary.8 When considering adherence in children, it is necessary to focus on ‘family adherence’. This is especially true in paediatric patients who had liver transplants, with more than two-thirds of patients below 2 years of age at the time of their first transplant.9
Numerous strategies have been developed with the aim of enhancing adherence in paediatric patients who had liver tranplants.8 Currently, family centred multidisciplinary care strategies seem to be the most effective in improving adherence to PTM.4 ,10 ,11 WHO has endorsed the implementation of pharmaceutical care within the patients’ care process,12 thus, pharmacists’ active involvement in patient-centred practice has increased in recent years with a positive impact on patient outcomes, such as improving adherence to medications.13 ,14 These concepts of family centred pharmaceutical care are well integrated in the patients’ care process at the Birmingham Children's Hospital (BCH) in the UK. The Liver Unit Transplant Programme undertakes 25–30 liver transplants annually, and supports a cohort of 750 patients. Every family receives family centred care, supported by a strong multidisciplinary team (paediatric liver surgeons, hepatologists, specialist nurses, pharmacists, dieticians, psychologists, physiotherapists, etc). At present, due to practicalities, the liver specialist nurse team is responsible for providing parents’ education and training in medicines. The pharmacy team is, however, extensively involved in the care process of patients who had liver transplants . A specialist clinical pharmacist is present on the ward each weekday, and a pharmacy team at BCH is responsible for the continuity of immunosuppressants supply when the patient is at home. This team of nine pharmacy staff provides a link between primary care, hospital and families in order to obtain prescriptions and medication supplies in time.
In Europe, the development of patient-centred medicine has increased in recent years.15 ,16 In the UK, government policy promotes an increased role for parents and children in decision making about treatment, reinforcing the importance of eliciting parents’ individual concerns.17 ,18 Taking into account the patients’ views has become a key point in the improvement of the quality of care.
The objective of this project was to identify the main medication issues encountered by children and their parents or carers, in order to identify care improvements. To support service development, a survey was conducted with parents or carers of paediatric patients who had liver transplants to identify their experiences and opinions of PTM management.
Material and methods
This study was an anonymised, single-site, multifactorial, cross-sectional study approved as ‘service development’ by the Research and Development Department of BCH.
Recruitment and data collection
Parents’ questionnaire survey
To obtain an accurate evaluation of parental experience, a questionnaire was developed. The survey was designed to be suitable for self-completion by the participants with direct support from the researchers. Open questions were included to allow individual comments. A cover letter explained the purpose of the study. To confirm that the questionnaire was understandable, a cognisance test was conducted with four parents. Following this evaluation, the questionnaire was slightly modified and approved by the study team.
The questionnaire was divided into nine parts: personal information, medicines and prescriptions, obtaining medicine supplies, giving your child medicines, medicines-related blood tests, side-effect (SE) management, opinion of hospital training and written information, opinion of proposed improvements and free comments (see appendix 1, web only file).
To target the critical period in terms of parents’ needs, the study population included parents of children who had received one or more liver transplant between January 2011 and May 2013.
Inclusion criteria: child living with the respondent; each parent (as a representative of the child) may only enter the study once—one parent only per child.
Exclusion criteria: respondent lacking English skills without an available interpreter.
Two ways were used to approach eligible participants. (1) Self-completion: parents were approached during outpatient clinic attendance over a period of 4 weeks during May 2013. The questionnaire was self-completed by parents with support, if necessary, from a study pharmacist. (2) Phone completion: a random selection of eligible parents were contacted by a pharmacy technician and pharmacist during a 2-week period in June 2013. Parents were informed about the study during the phone interviews. Parents’ answers were transcribed verbatim prior to analysis. Eligible participants who had already been approached following the clinic attendance were not contacted by phone.
The randomisation facility in MS Excel 2010 (RAND) was used to select the study cohort from the 48 eligible patients who were contacted by telephone. After three unanswered calls, parents were considered as non-respondents.
Mails and phone calls database
Post-transplant parents can contact specialist nurses by mail or phone using the Liver Direct Help Line 24/7 (LDHL). Queries are relayed to the healthcare professional concerned (pharmacist, dietician, hepatologist, etc) to facilitate specialised support. The event is recorded in the Liver Database (LD).
The records in the LD for the questionnaire survey participants were identified and classified in three areas: clinical, medications, and other fields—in order to establish the proportion of interventions related to medications. The main medication issues were identified for the study cohort.
Medical clinic letters
After every medical consultation, a letter is written by the consultant and registered in the LD. These letters contain information on patient's clinical progress, including a section on medicines. Medication issues in letters for the study cohort were identified.
Data analysis
The questionnaires used for the in-clinic self-completion and phone completion are materially the same, and data was pooled. All data were analysed using MS Excel 2010.
Results
Population characteristics
Thirty-seven parents were recruited, which represents 77.1% of children transplanted between January 2011 and May 2013 (figure 1). The proportion of boys was 59.5%. Mean age was 5.67 years (CI 95 (4.14 to 7.19)), and the mean time since transplantation corresponded to 1.32 years (CI 95 (1.10 to 1.54)).
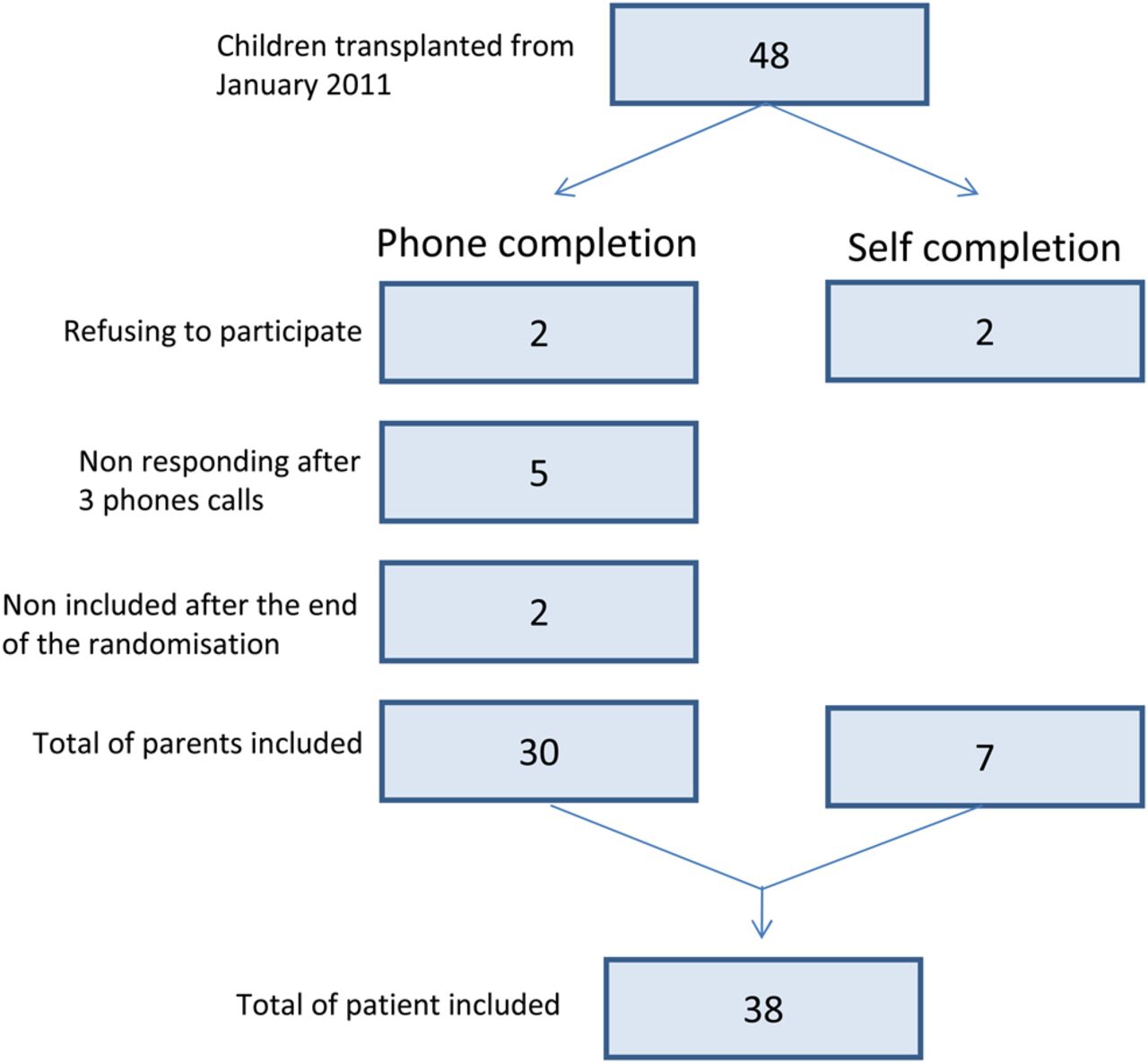
{kind=link}
Recruitment strategy.
Medication issues
Questionnaire data
All questionnaires were entirely completed, with no omissions.
Medicines and prescriptions
In the last 3 months, an average number of 5.19 medicines were prescribed per child (CI 95 (4.30 to 6.07)). Most parents received a combination of general practitioners’ (GP) and hospital doctors’ prescriptions. Medicine supplies were mainly managed by the hospital pharmacy Clinical Interface Liaison Team, and supplied either by a homecare company or community pharmacies, or both (table 1).
Medicine prescriptions and deliveries
Obtaining their child's medicines
In the last year, 32.4% (n=12) of parents had experienced a total of 17 medication supply problems: one supply problem (n=8); two supply problems (n=3); three supply problems (n=1).
The most frequent problem was that the GP refused to prescribe the medicine(s) (table 2).
Issues encountered regarding medication supply
To the question ‘In the last 12 months, approximately how many times did you actually run out of medicine?’, 81.1% (n=30) of parents answered ‘1 to 12 times’. However, only one child missed a medication dose (a vitamin dose that was not supplied in time). No child missed a dose of immunosuppressant.
Giving medicines to their child
Most parents reported a good understanding of why each medicine was prescribed (59.7% very well, 29.4% well, 8.1% ok). Three parents experienced problems when measuring out the dose (26 children were taking liquids). There were difficulties in obtaining oral syringes which measure the exact volume of the dose.
Nine parents experienced problems when they gave the medicine to their child. The most frequent issue was vomiting (n=7).
Medicine-related blood tests
Most respondents had a good understanding of why immunosuppressants need to be monitored using blood tests (78.4% very well, 13.5% well, 8.1% ok), and why they must not be given before the blood test (64.9% very well, 27.0% well, 8.1% ok).
There were 37.8% (n=14) of parents who experienced problems with blood tests (only 1–12 times in the last year). The most frequent difficulty was obtaining results (n=6) (see supplementary table, web only file).
Side-effect management
There were 56.8% (n=21) of children who had SEs during the last year, according to their parents (eg, headache, hypertension, hypertrichosis). Most respondents reported good knowledge of how to manage SE (29.7% very well, 29.7% well, 37.8% ok and 2.7% poorly).
Parents’ opinion of hospital training and documentation
Most parents had an excellent or very good opinion of the training (81.1%, n=30) and quality of written information provided (67.6%, n=25).
All parents thought that all the information provided was understandable, and 97.3% (n=36) reported that all the information they needed was provided. Only one parent felt that the time available to talk about medicines was too short. Similarly, concerning the quality of the documentation, 97.3% (n=36) of parents thought that all the information provided was understandable and complete. One parent disagreed because of a lack of English reading skills.
Parents’ opinion of proposed improvements
Five proposed service improvements were described in the questionnaire (see table 3).
Parents’ opinion of the helpfulness of the five proposed improvements
Free comments
Totally, 21.6% of respondents made a free text comment. Most related to the proposed improvements (see appendix 2, web only file).
Liver direct help line data
According to the questionnaire, in the last year, 35.1% of parents declared in the questionnaire that they had never contacted the LDHL for medication questions; 56.8% of them only 1–12 times and 8.1%, 25–52 times. Of the 64.9% (n=24) of parents who declared having contacted LDHL, 91.7% of them always obtained an answer to their queries, and the remaining 8.3% most of the time.
Totally, 34 parents actually contacted the LDHL during the study period (total number of enquiries=257). The majority of parents’ enquiries were related to medication (n=167, table 4). Except for parents’ enquiries to inform the Liver Team that the blood test had been done (n=44), all other medication-related enquiries were parents’ medication issues (n=123, for 26 parents). Thus, medication issues represented approximately 4.7 enquiries per family.
Summary of parents’ enquiries related to medication
Medical clinic letters data
Ninety-nine letters were analysed; 18.2% (n=18) reported a medication issue. The majority of the issues were related to SE management (eg, child Cushingoid due to prednisolone—dose was reduced) (table 5).
Medication issues reported in clinic letters
Discussion
Medication issues
The LD analysis provided an overview of parents concerns and showed that medication issues were most frequent. Approximately one-third of participants reported medication problems in each category (obtaining their child's medicines, medicine-related blood tests, etc). However, frequency of medication issues per family was low. Indeed, each category of issue was rarely reported outside the range of 1–12 times a year in the questionnaire survey. This was reinforced by the LDHL database with less than five interventions per family per year regarding medication issues. This emphasises the effectiveness of family centred multidisciplinary care implemented as previously reported.4 ,11 ,12
Parents reported a refusal from the GP to prescribe an unlicensed medicine (eg, immunosuppressant). This observation is similar to that of a study conducted in another English paediatric hospital about supply problems of unlicensed medicines after discharge.19 These supply difficulties explain the large number of prescriptions written by hospital prescribers, and the necessity of having a homecare company to manage unlicensed product deliveries in the UK. Homecare companies specialise in ‘dispense and deliver’ medication services at the request of either hospital prescribers or GPs. This may be particularly useful for complex or uncommon medicines needed on an on-going basis (eg, unlicensed medicines for children). Although 81.1% parents had almost run out of medication, the fact that no patient missed an immunosuppressant dose demonstrated that close cooperation within the multidisciplinary team is effective in preventing missed doses of important drugs. A continuous medication supply is achieved in large part due to the Commissioning and Interface Liaison Team (CILT), a subdepartment of BCH pharmacy. This team of nine pharmacy staff coordinates the medication supply arrangements, including the provision of prescriptions and their dispensing. CILT provides a link between primary care, hospital and families in order to obtain prescriptions and medication supplies in time.
Problems giving medication were infrequent (n=3), and related to obtaining oral syringes. While community pharmacists in the UK are contractually required to provide the means to take medicines they dispense, oral syringes are neither prescribable nor reimbursed, and it is not current practice for community pharmacists to provide them. A possible solution to help parents to obtain oral syringes is to ask the homecare company to provide them at the same time as the medicines.
More than half the parents reported that their child experienced drug-related SE in the last year. This is also the most frequent point discussed in medical clinic letters. Furthermore, parents seemed less confident in their knowledge of SE management, compared with their understanding of blood test management, or of the role of each medicine. Further development of SE information sessions should be considered to reassure parents (eg, hypertrichosis and cyclosporin). The clinical specialist pharmacist could provide these SE information sessions during pharmaceutical consultations scheduled for the same day as medical consultations.
Parents’ opinions on current practice and proposed improvements
Parents were particularly satisfied with medical information they received. Nevertheless, one parent commented that the time accorded to PTM management was too short, with not enough detail. This should be considered in service development plans and may be a role for pharmacy staff.
Creation of an online learning tool was the most popular proposed improvement. These ‘e-Health’ tools are applications of technology expected to either improve a patient's understanding of health information or to be used as an aid for health professionals in care delivery.20 The proposed comic book, intended to explain transplantation and medicines, was also highly popular. This could help parents when explaining issues to their child, and be a useful addition to sessions with hospital play specialists and psychologists.8
The suggestion of increasing pharmacist involvement was well received by parents. The establishment of pharmaceutical consultations, scheduled for the same day as medical consultations, could support parents who want to have further information on PTM management. The content of the pharmaceutical consultation could be tailored to each particular family's needs.
Nevertheless, medication issues may occur between follow-up consultations and, with increased time post-transplantation, patients may return to clinic infrequently, making a face-to-face intervention less likely. The LDHL is currently the only non-scheduled method used by parents to obtain help. This appeared to be effective, given that almost all parents always obtained an answer to their requests. However, specialist pharmacists with their expertise in PTM may be well placed to answer medication-related queries. That is why providing the email address of a specialist pharmacist in addition to the LDHL could be a suitable solution, especially as many parents reported that this idea would have a very high benefit.
Limitations
This present study has a number of limitations. Although the investigation represents a nearly complete survey of one centre's eligible population (77.1%), this is still a small number of single-site patients, and generalisation of the results to other post-transplant patients is limited.
As the study instrument was a questionnaire survey, results are based on what respondents told us, which may not have fully reflected what they actually experienced. Although the categories chosen to obtain frequency of issues were based on the calendar to aid memory, they appeared to not be fully relevant to all questions. More issues were expected to be reported by parents. Results obtained suggest that narrower frequency groups would have been useful.
Finally, our study population, covering a period of 0–2 years post-transplant, only allowed a cross-sectional assessment, and no attempt was made to consider changes over time. Further longitudinal studies are warranted to identify time-dependent changes.
Conclusion
This study evaluates three sources of information (parents’ questionnaire, LDHL and medical letters) to audit the process of care. This is the first published parent survey about PTM management. This work has improved our understanding of the issues encountered, and also supports identifying the parents’ perspective in order to evolve our practice according to their real needs.
In the early years post-transplantation, parents experienced issues linked to medication supply, medication administration process, medicine-related blood tests and/or SE management. A lot of support is provided by the study-site multidisciplinary team to support families with this complex medication management, and parents seemed particularly satisfied by the current training and documentation about medicine. Nevertheless, some improvements could be made in order to best serve children and their parents. Among the suggestions favoured by the parents were: an online learning tool, a comic book and providing further access to pharmacists.
A multidisciplinary working group, including a parent representative, will be established in our centre to consider these potential service improvements.
Key messages
What is already known on this subject
-
Post-transplant medications (PTM) are often considered a challenge that can sometimes be difficult to manage for young patients and their parents or carers.
-
Non-adherence to PTM is an important issue for paediatric patients who had transplants.
-
Family centred multidisciplinary care strategies seem to be the most effective in improving adherence to PTM.
What this study adds
-
The study provides information on PTM issues of parents and carers of patients who had liver transplants.
-
This work highlights the importance of identifying parents’ perspective in order to evolve family centred care according to their real needs.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table
Footnotes
-
Contributors LG conducted the project supervised by DT, AR, AD and KS.
-
Competing interests None.
-
Ethics approval Research and Development Department of BCH.
-
Provenance and peer review Not commissioned; externally peer reviewed.