Article Text

Abstract
Piperacillin/tazobactam is a bacteriolytic combined antibiotic. The least common reported adverse reactions of piperacillin/tazobactam are haematological reactions (<1%). The use of piperacillin/tazobactam during pregnancy is considered to be moderately safe (pregnancy category B) for the human embryo-foetus. This is a case of a pregnant patient (22 weeks of gestation) who was admitted to the Women’s Hospital, Doha, Qatar and was treated for preterm premature rupture of membrane with erythromycin for 10 days. Afterwards, she was treated with piperacillin/tazobactam for asymptomatic urinary tract infection (pseudomonas species). After 15 days, she developed fever, leucopenia, neutropenia and thrombocytopenia. These adverse reactions were reversed after the discontinuation of piperacillin/tazobactam combination. In Qatar and worldwide, there are few reported cases regarding bone marrow suppression or fever induced by piperacillin/tazobactam in general and during pregnancy. Using the Naranjo Adverse Drug Reaction Probability scales, the score was found to be 8, representing a probable adverse drug reaction.
- bone marrow suppression
- piperacillin/tazobactam
- pregnancy
- qatar
- thrombocytopenia
Statistics from Altmetric.com
Background
Piperacillin/tazobactam is a bacteriolytic combined antibiotic that contains the extended-spectrum penicillin antibiotic, piperacillin and the β-lactamase inhibitor, tazobactam.1 2 Piperacillin binds to penicillin-binding proteins which, in turn, inhibits bacterial cell wall synthesis and then inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls, thus inhibiting cell wall biosynthesis.1 2 The piperacillin/tazobactam combination has activity against Staphylococcus aureus (methicillin susceptible), Coagulase negative Staphylococci, Streptococcus pneumoniae (penicillin susceptible), Streptococcus spp., Haemophilus influenzae, Moraxella catarrhalis, Neisseria meningitides, Neisseria gonorrhoeae, Enterobacteriaceae, E. coli and Pseudomonas aeruginosa.1–3 In the general population, the use of piperacillin/tazobactam combination is considered to be safe.2 4 The most common adverse reactions are diarrhoea (7% to 11%), and Clostridium difficile-associated diarrhoea (4.9%).2 4 The use of piperacillin/tazobactam combination was reported in some case reports (non-pregnant patients) to induce fever, neutropenia and bone marrow suppression (leucopenia, thrombocytopenia).5 6 Bone marrow suppression or myelosuppression is the decrease in production of leukocytes (leucopenia), thrombocytes (thrombocytopenia) and/or erythropenia.
Piperacillin/tazobactam combination is a derivative of penicillin nucleus and there is a considerable experience with penicillin in human pregnancy.5–7 Thus the use of piperacillin/tazobactam combination during pregnancy is considered to be moderately safe for the human embryo-foetus.7 A literature search of standard databases (Medline, PubMed and Embase) was conducted in October 2016 and it did not identify similar reports during pregnancy. Accordingly, in Qatar and worldwide, there are no reported cases regarding any form of bone marrow suppression and/or fever induced by piperacillin/tazobactam combination during pregnancy. We report the first case report of fever, leucopenia, neutropenia and thrombocytopenia induced by piperacillin/tazobactam combination during pregnancy. This is a descriptive case report and a waiver of informed consent and ethical approval were obtained from Hamad Medical Research Centre, Hamad Medical Corporation, Qatar.
Case presentation
A pregnant patient in her thirties (22 weeks of gestation, gravid 6 para 3 plus two miscarriages) was admitted to the Women’s Hospital. Her previous obstetric history was remarkable for one neonatal death due to interventricular haemorrhage and two second trimester miscarriages. Her previous surgical history included two documented lower segment caesarean sections. Her previous medical history was unremarkable. She had no history of drug allergies or adverse drug reactions.
Prior to admission, she was taking progesterone vaginal suppository (400 mg twice daily), iron fumarate tablet (65 mg elemental iron twice daily) and ranitidine tablet (150 mg once daily). In her current pregnancy, she had regular antenatal follow-ups and she had cervical cerclage at 14 weeks. On admission, she was assessed by the specialist obstetrician. She was conscious, well-oriented to time, place and person and she was afebrile and vitally stable. The abdomen was soft, lax and not tender. Cervical speculum examination identified positive clear liquor, closed cervical os and cervical cerclage in situ. Ultrasound revealed no amniotic fluid volume, anhydramnios with no fluid pocket seen. Based on subjective and objective measures, she was diagnosed with preterm premature rupture of membrane (PPROM). The hospital management protocol for PPROM was followed, and the patient received erythromycin oral tablets (250 mg every 6 hours for 10 days). As an in-patient, she continued progesterone vaginal suppository, iron, and ranitidine.
The primary obstetrician team discussed with the patient her condition and explained to her the potential foetal outcomes (prematurity) and maternal risks (chorioamnionitis). The patient refused either terminating the pregnancy (delivering the foetus) or removing the cerclage stitch. Consequently, the patient was managed conservatively and was kept as an in-patient and she was informed that if any sign of infection appeared the pregnancy would be terminated. As per the hospital protocol, complete blood count (CBC), high vaginal swab, and urine culture were repeated twice weekly. The vital signs were monitored on a daily basis. At 24 weeks of gestation, intramuscular betamethasone was administered (12 mg every 24 hours for 2 days) for neonatal lung maturation as a precaution in case of a preterm delivery. She was started on subcutaneous enoxaparin (40 mg once daily) as a venous thromboembolism prophylaxis.
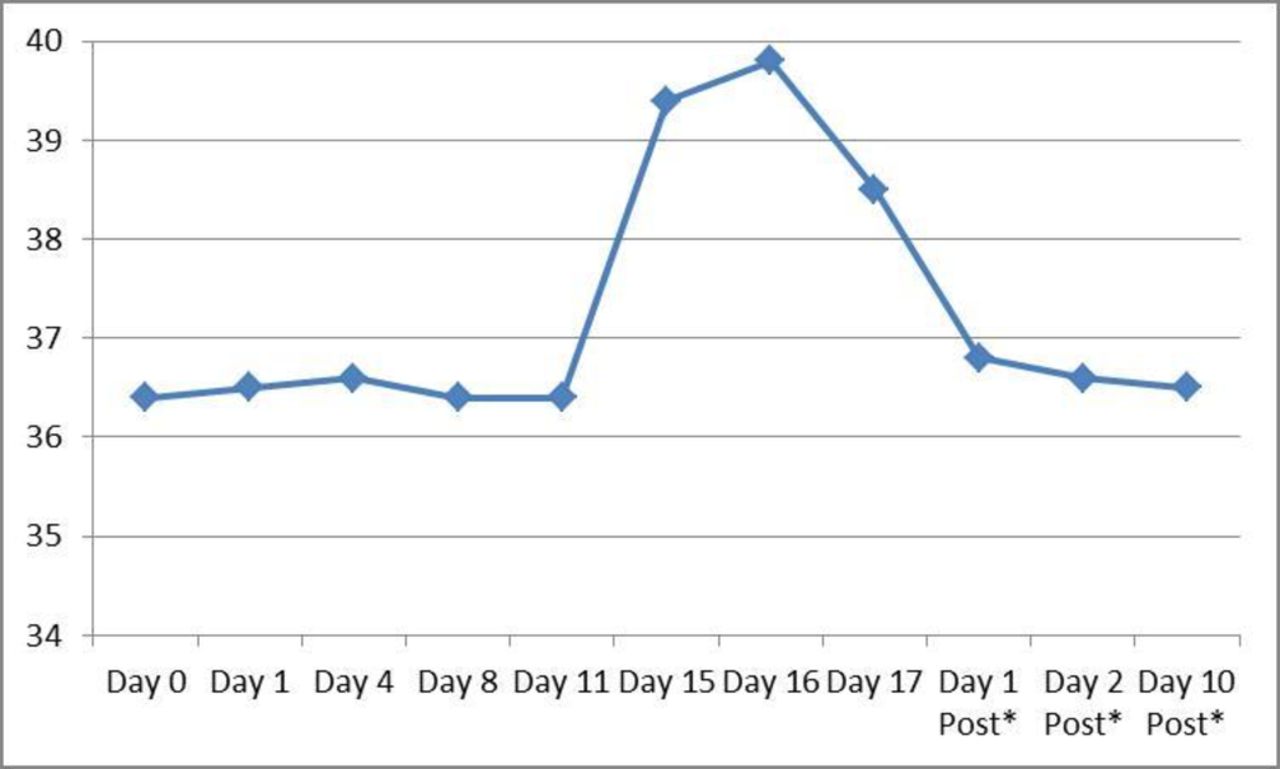
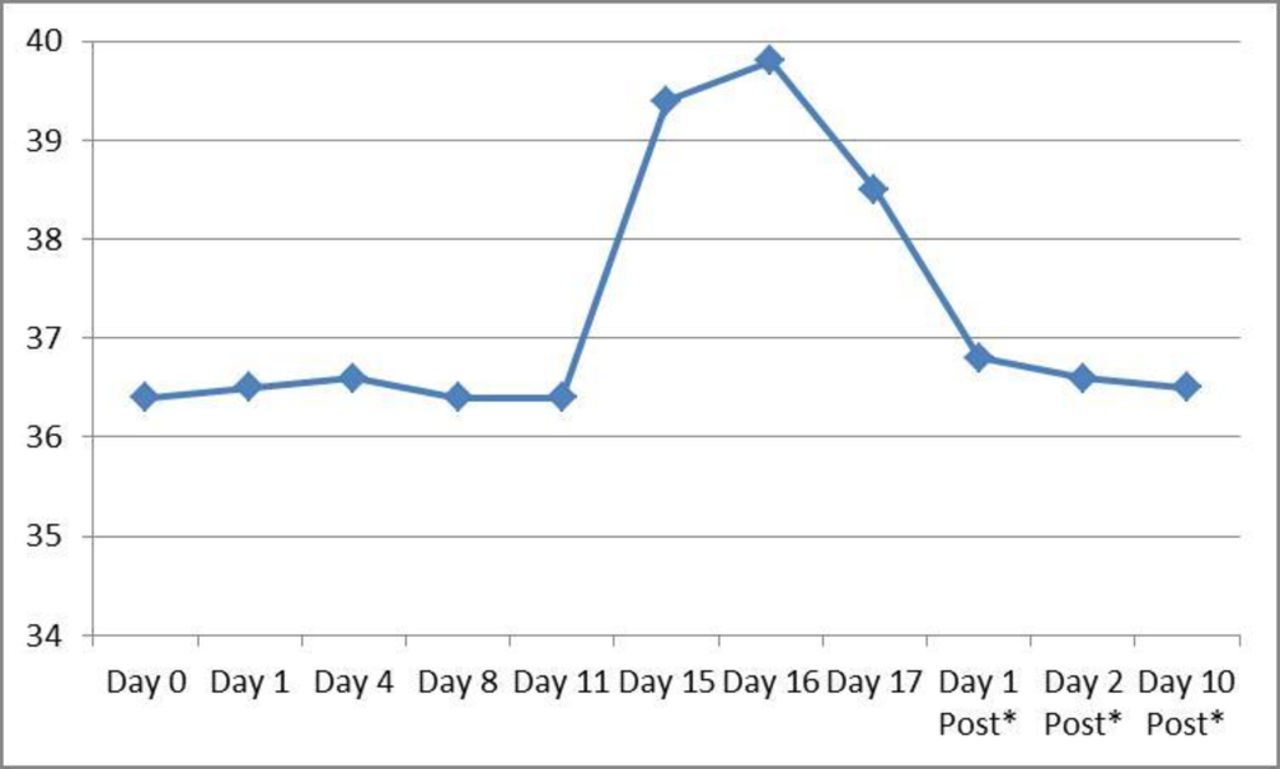
After 24 days of PPROM (25 weeks of gestation), the urine culture revealed mixed growth including Pseudomonas species, but the patient was asymptomatic. The infectious disease team was consulted and they decided to prescribe intravenous piperacillin/tazobactam combination (4.5 gm every 8 hours until delivery), antibiotic day 1. The patient’s vital signs and haematological parameters were monitored continuously and all were within normal range until antibiotic day 14. On antibiotic day 15, the patient started to have low-grade fever (37.8°C) and the white blood cells (WBCs), neutrophils and platelets were declining compared with the preceding days. On antibiotic day 16, the patient continued to have fever (39.8°C) and the WBCs, platelets and neutrophils declined further, and the values were less than the normal. On antibiotic day 17, the patient’s medical status continued to deteriorate with fever (>38°C), leucopenia (critical value of WBCs 1.4×103/ µL), neutropenia (neutrophils 0.9×103/ µL), and thrombocytopenia (platelets 45×103/ µL). Haematological parameters and temperature charting are given in figures 1 and 2, respectively.
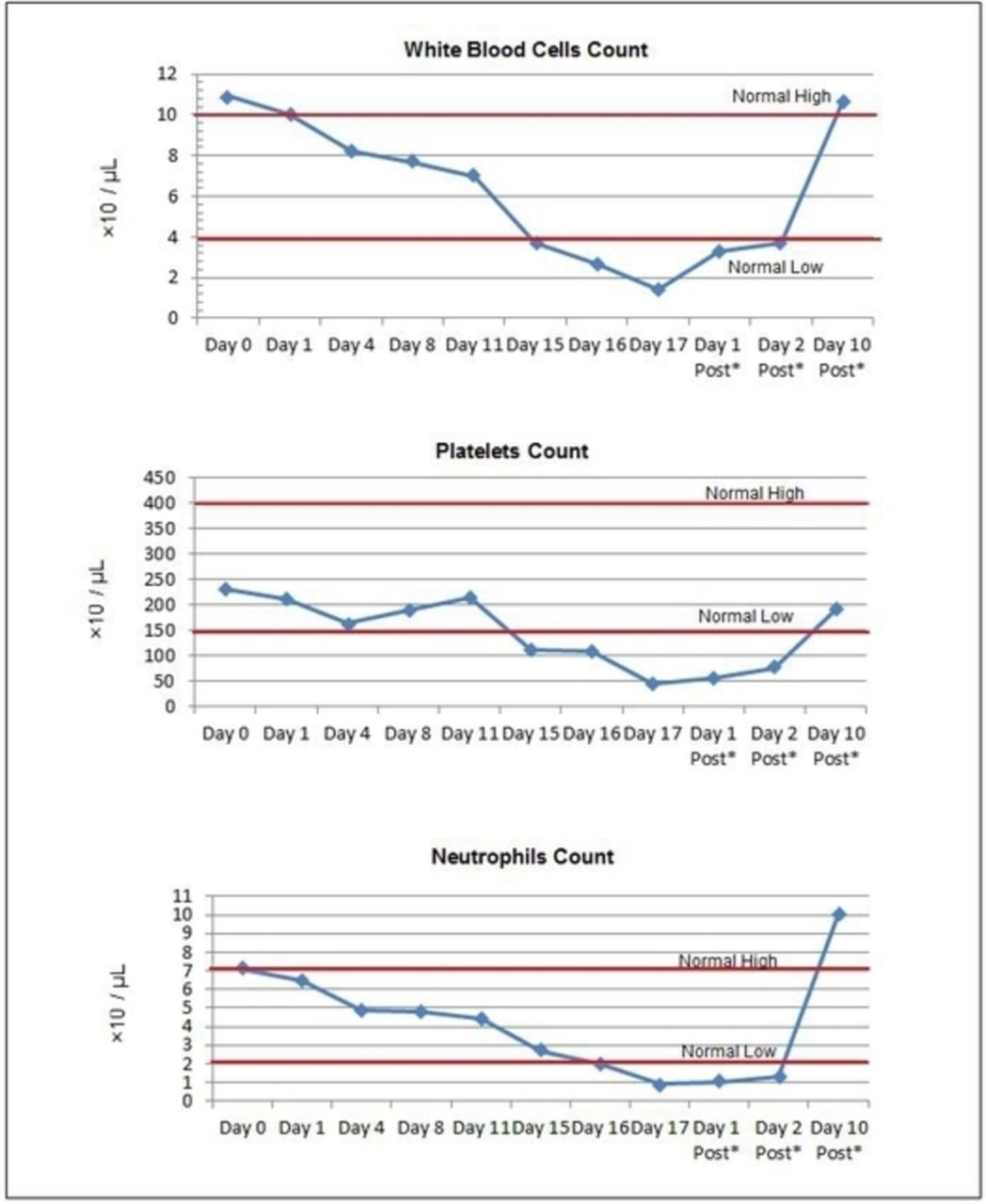
White blood cells, platelets and neutrophils count during the course of therapy and post antibiotic discontinuation.
{kind=link}
{kind=link}
Temperature charting during the course of therapy and post antibiotic discontinuation.
On antibiotic day 17 (28 weeks of gestation), the possibility of chorioamnionitis (intra-amniotic infection) was highly suspected by the primary obstetrician team, and this was based on the patient’s haematological parameters and temperature charting. The primary care obstetrician team discussed with the patient her current situation and they discussed the high possibility of chorioamnionitis; thus the decision was made for emergency lower segment caesarean section (LSCS). The decision of LSCS was influenced by, mainly, the effects of chorioamnionitis on the mother and foetus. The baby was delivered at 28 weeks of gestation. During the LSCS, the delivered placenta was sent for histopathology investigation and culture in order to confirm or exclude chorioamnionitis diagnosis.
After 24 hours of childbirth via LSCS, piperacillin/tazobactam combination was discontinued, as the possibility of antibiotic- induced adverse drug reaction was highly suspected. Day three post-LSCS and day two post-discontinuation of piperacillin/tazobactam combination, the haematological parameters (WBCs, platelets, neutrophils) and fever started to normalise. On day 28 post-discontinuation of piperacillin/tazobactam combination, the haematological parameters (WBCs, platelets, neutrophils) and temperature were normal (figures 1 and 2). The placental histopathology showed immature chorionic villi with no established chorioamnionitis. Furthermore, placental culture showed moderate polymorphonuclear leukocytes without epithelial cells and organisms' growth (negative placental culture). Based on the results of the placental histopathology and culture, the possible diagnosis of chorioamnionitis was completely excluded.
Investigations
The chorioamnionitis diagnosis is based on clinical findings and some objective measures. Diagnosis can be made if maternal oral temperature is ≥39.0°C or between 38.0°C and 39.0°C on two occasions. In addition, one of the following shall be present, baseline foetal heart rate >160 beats/min for ≥10 min, maternal WBC>15×103/ µL in the absence of corticosteroids, purulent-appearing fluid coming from the cervical os visualised by speculum examination.2 Diagnosis can be confirmed by the presence of the above mentioned criteria plus one or more objective laboratory findings such as low glucose level in amniotic fluid, positive amniotic fluid culture, high WBC in amniotic fluid, histopathologic evidence of infection in the placenta, foetal membranes or the umbilical cord vessels.2 Prior to childbirth and LSCS, the diagnosis of chorioamnionitis was not confirmed. This is mainly because the patient’s laboratory and clinical factors were not all in accordance with the diagnosis of chorioamnionitis. After childbirth, the placental histopathology showed immature chorionic villi with no established chorioamnionitis. Furthermore, placental culture showed moderate polymorphonuclear leukocytes without epithelial cells and organisms' growth (negative placental culture). Based on the results of the placental histopathology and culture, the possible diagnosis of chorioamnionitis was completely excluded.
Outcome and follow-up
After 24 hours of childbirth via LSCS, piperacillin/tazobactam combination was discontinued, as the possibility of antibiotic-induced adverse drug reaction was highly suspected. Day three post-LSCS and day two post-discontinuation of piperacillin/tazobactam combination, the haematological parameters (WBCs, platelets, neutrophils) and fever started to normalise.
Discussion
This is the first published case report of fever, leucopenia, neutropenia and thrombocytopenia induced by piperacillin/tazobactam combination during pregnancy. Using the Naranjo Adverse Drug Reaction Probability scales, the score was found to be 8, representing a probable adverse drug reaction.
In this case report, the patient started to have fever, leucopenia, neutropenia and thrombocytopenia on day 15 of piperacillin/tazobactam combination. This is similar to the previous reports, where the adverse effects begun 11 to 17 days after the initiation of piperacillin/tazobactam combination.8 9 This patient received a total daily dose of 13.5 gm of piperacillin/tazobactam combination. In addition, the total cumulative piperacillin/tazobactam combination over the course of therapy was 3050 mg/kg body weight. The received cumulative dose is within the previously reported cumulative dose range which caused bone marrow suppression, piperacillin/tazobactam cumulative dose of 4919±1975 mg/kg body weight.8
Previous case reports of piperacillin/tazobactam combination-induced fever and bone marrow suppression has occurred in young or elderly male patients.5 6 In Qatar and worldwide, there are few reported cases regarding bone marrow suppression or fever induced by piperacillin/tazobactam in general and during pregnancy. In this patient, the adverse drug reactions occurred 15 days after the initiation of piperacillin/tazobactam combination and promptly reversed with the discontinuation of the medication. Health-care professionals should be attentive of these serious adverse drug reactions, because these may have serious implications for both mother and foetus.
Chorioamnionitis (intra-amniotic infection) is an infection of the amniotic fluid, foetus, umbilical cord or placenta.2 Prior to childbirth and LSCS, the diagnosis of chorioamnionitis was not confirmed. This is mainly because the patient’s laboratory and clinical factors were not all in accordance with the diagnosis of chorioamnionitis. However after childbirth and LSCS, the possible diagnosis of chorioamnionitis was completely excluded as the placental culture came out to be negative.
In conclusion, we report a case of probable fever, leucopenia, neutropenia and thrombocytopenia induced by piperacillin/tazobactam combination in a pregnant woman. It is important for health-care professionals to be aware of the possibility of these serious adverse drug reactions while treating patients using this antibiotic combination. All patients must be monitored carefully while being treated with this combination, especially during pregnancy.
Learning points
This is the first published case report of fever, leucopenia, neutropenia and thrombocytopenia induced by piperacillin/tazobactam combination during pregnancy
The use of Naranjo Adverse Drug Reaction Probability scales shall be considered in accessing the probability of any suspected adverse drug reaction
The score of Naranjo Adverse Drug Reaction Probability scales in this case report was found to be 8, representing a probable adverse drug reaction
As health-care professionals, it is important to be aware of the possibility of these serious adverse drug reactions while using this antibiotic combination (piperacillin/tazobactam)
Footnotes
Selsalem S, et al
Contributors SES and SE: overall case interpretation and manuscript writing. AA, MAS and MAH: results interpretation. SES: manuscript submission and modification.
Ethics approval Hamad Medical Research Centre, Hamad Medical Corporation, Qatar.
Patient consent for publication The patient’s consent could not be obtained because the patient was no longer living in the country and her contact details were not readily available. A waiver of informed consent was granted by the Institutional Review Board (IRB) for publication of this case.