Article Text

Abstract
Aims To perform a pharmaco-economic analysis of prescribing alternative antibiotics in patients with a diagnostic label of ‘penicillin allergy’ and assess whether collation of information from a structured history and liaison with the family physician could reduce costs.
Methods A prospective pro-forma-based interview of randomly selected in-patients and their family physician was used to assess the validity of the diagnostic label of ‘penicillin allergy’. Cost analysis of prescription of alternative antibiotics was performed and compared with first-line agents.
Results 102 patients were assessed and only 40% (n=41) were found to have a history consistent with penicillin hypersensitivity, 40% (n=41) were likely ‘not allergic’ and 20% (n=20) had ‘indeterminate’ reactions. Total cost of antibiotics prescribed for patients with penicillin allergy was 1.82–2.58-fold higher than for first-line antibiotics.
Conclusions Obtaining a structured history from the patient and family physician alone can enable an accurate identification of penicillin allergy status. Total acquisition cost of second-line antibiotics is higher than if these patients were prescribed first-line antibiotics.
- ANAPHYLACTIC REACTIONS
- ANTIBIOTICS
- IMMUNOLOGY
Statistics from Altmetric.com
Introduction
Penicillin-based antibiotics are first-line treatment for common infections, and the diagnostic label of ‘penicillin allergy’ precludes usage in routine clinical practice and second-line therapy is often employed. Previous data suggest that only <10% of these patients are ‘truly allergic’ following formal evaluation.1–3
Using non-β-lactam antibiotics in certain infections has been shown to be less efficacious including vancomycin monotherapy for Staphylococcus aureus bacteraemia, which is associated with higher mortality rates.4
There is paucity of data relating to pharmaco-economic analysis, and a Danish study reported that acquisition of alternative antibiotics for a patient allergic to penicillin is 2.3-fold higher.5
Fluoroquinolones, carbapenems and clindamycin are usually employed as alternatives to penicillin and are associated with greater risk of Clostridium difficile colitis,6 which may increase mortality, hospital stays and overall costs. Carbapenem use can also further increase the selection pressure for carbapenemase-producing Enterobacteriaceae.7
The main objective of this study was to prospectively evaluate patients with a diagnostic label of penicillin allergy by obtaining a structured clinical history (from the patient and their family physician) and to clinically ascertain the likelihood of hypersensitivity and to evaluate downstream financial cost of prescribing non-penicillin-related antibiotics.
Patients and methods
Patient selection
Patients admitted to Heart of England NHS Foundation Trust (HoEFT) between 6 November 2012 and 27 February 2013, with a diagnostic label of ‘penicillin allergy’, were identified using the hospital electronic prescribing (EP) system.
A daily report was generated from the EP system that listed all wards and all patients on antibiotics across three acute-care hospitals that formed HoEFT. The report highlighted patients with a diagnostic label of penicillin allergy.
Patients with a label of penicillin allergy on the EP report were included on a ward-by-ward basis. A new report was generated each day and all patients were selected from wards that were not covered from the previous day. This process was continued until all wards were covered and the cycle was repeated. All patients enrolled were interviewed by the same clinician.
Paediatric, acute stroke, intensive care and cystic fibrosis patients were excluded from selection. This was due to the high likelihood of having to rely on clinical history from a relative.
Cognitive function was assessed using Abbreviated Mental Test (AMT) score. The AMT score is a set of 10 questions developed by Hodkinson for the rapid assessment of dementia in elderly patients.8 A ‘cut-off’ score of 8 is used to discriminate between cognitive impairment and normality.9 Patients who scored lower than 8 were excluded from the study. Patients that had been assessed with the shortened version of AMT, called AMT 4, and scored lower than 3 were also excluded.10
Categorisation of patients as per clinical history
A standardised pro-forma (see online supplementary appendix 1) was employed to obtain the history surrounding the diagnosis of penicillin allergy. This included details regarding nature of rash, whether there were associated cardiorespiratory and gastrointestinal symptoms, rapidity of onset and temporal association with administration of the antibiotic.
The pro-forma was extended to allow input from the family physician via telephone interview and covered the above information. Date of most recent prescription of a β-lactam antibiotic was also included.
Based on clinical history, patients were categorised into ‘immediate’ (type 1) hypersensitivity reactions and ‘non-immediate’ hypersensitivity reactions, based on European Network of Drug Allergy recommendations,11 ,12 and ‘non-allergic’ or ‘indeterminate’. Onset of allergy symptoms consistent with urticaria, angioedema, bronchospasm or hypotension after the first dose or <1 h following administration was considered immediate. Patients who reported onset of reactions after 1 h or during the course of penicillin/aminopenicillin were classed as non-immediate reactions.
Patients were deemed ‘non-allergic’ if:
-
They did not declare an allergy to penicillin and confirmed accordingly by the family physician.
-
They reported an allergy but subsequently received penicillin/aminopenicillin with no recorded reaction.
-
The symptoms were not consistent with immediate or non-immediate hypersensitivity reactions.
Patients who failed to describe the nature of symptoms and where there was no further information from the family physician's records were classed as ‘indeterminate’.
Details of alternative antibiotics and infections
Data including nature of infection, type of antibiotic used, route of administration and duration of therapy during the patient's entire in-patient admission were collated. Cost of alternative antibiotics prescribed for each patient were calculated and compared with first-line antibiotics (table 1) that could have been employed. The cost of each antibiotic was deduced from the British National Formulary September 2012 edition.
First-line antibiotics and durations used in cost comparison analysis
Since there was no standardised time with respect to when patients were switched from intravenous to oral formulations, costs were calculated first with the assumption that all antibiotics with both oral and intravenous formulations were used orally. Second, that all antibiotics with both oral and intravenous formulations were used intravenously. In patients with an infection that could only be treated with intravenous therapy such as endocarditis, only intravenous antibiotic cost was included. Prophylactic antibiotics were excluded from cost calculations unless commenced during current admission.
The total cost of the antibiotics prescribed to each patient and total cost of first-line antibiotics that could have been employed were calculated according to criteria listed in table 2.
Criteria used to calculate total costs of antibiotics prescribed and first-line antibiotics
Criterion 1 was calculated as cost of antibiotics and for durations that were actually prescribed. This assumes all antibiotics with intravenous and oral formulations were used as intravenously.
Criterion 2 was calculated as cost of antibiotics and for durations that were actually prescribed. This assumes all antibiotics with intravenous and oral formulations were used as oral.
Criterion 3 was calculated as if first-line antibiotics had been used with guideline durations. This total assumes all antibiotics with intravenous and oral formulations were used as intravenously.
Criterion 4 was calculated as if first-line antibiotics had been used with guideline durations. This assumes all antibiotics with intravenous and oral formulations were used as oral.
Criterion 5 was calculated as if first-line antibiotics had been used but for the same durations as the prescribed antibiotics (ie, durations used in criteria 1 and 2). This assumes all antibiotics with intravenous and oral formulations were used as intravenously.
Criterion 6 was calculated as if first-line antibiotics had been used but for the same durations as the prescribed antibiotics (ie, durations used in criteria 1 and 2). This assumes all antibiotics with intravenous and oral formulations were used as oral.
The comparison first-line antibiotics were referenced from local HoEFT guidelines (table 1).
First-line antibiotics also included those recommended by infectious diseases or microbiology teams based on sensitivity testing. Standard adult doses taken from the British National Formulary were assumed except in endocarditis and deep-seated staphylococcal infection where costs were calculated based on higher doses and/or frequency. Standard dosage for antibiotics (with more variable doses) were taken as 600 mg daily for teicoplanin; 1 g twice daily for vancomycin, 500 mg daily for daptomycin, 450 mg four times daily for oral clindamycin; 600 mg four times daily intravenous clindamycin and 320 mg once daily for gentamicin (80 mg twice daily for endocarditis).
Duration for endocarditis and bone and joint infections were as per previously published guidelines.13 ,14
Results
Demographics
A total of 165 patients were identified across three hospitals; their inclusion and outcomes are summarised in figure 1. After exclusion (figure 1), 102 patients were enrolled into the study. This included 46 male and 56 female patients, with a median age of 75.5 years (Q1–Q3, 63.3–83.0 years).
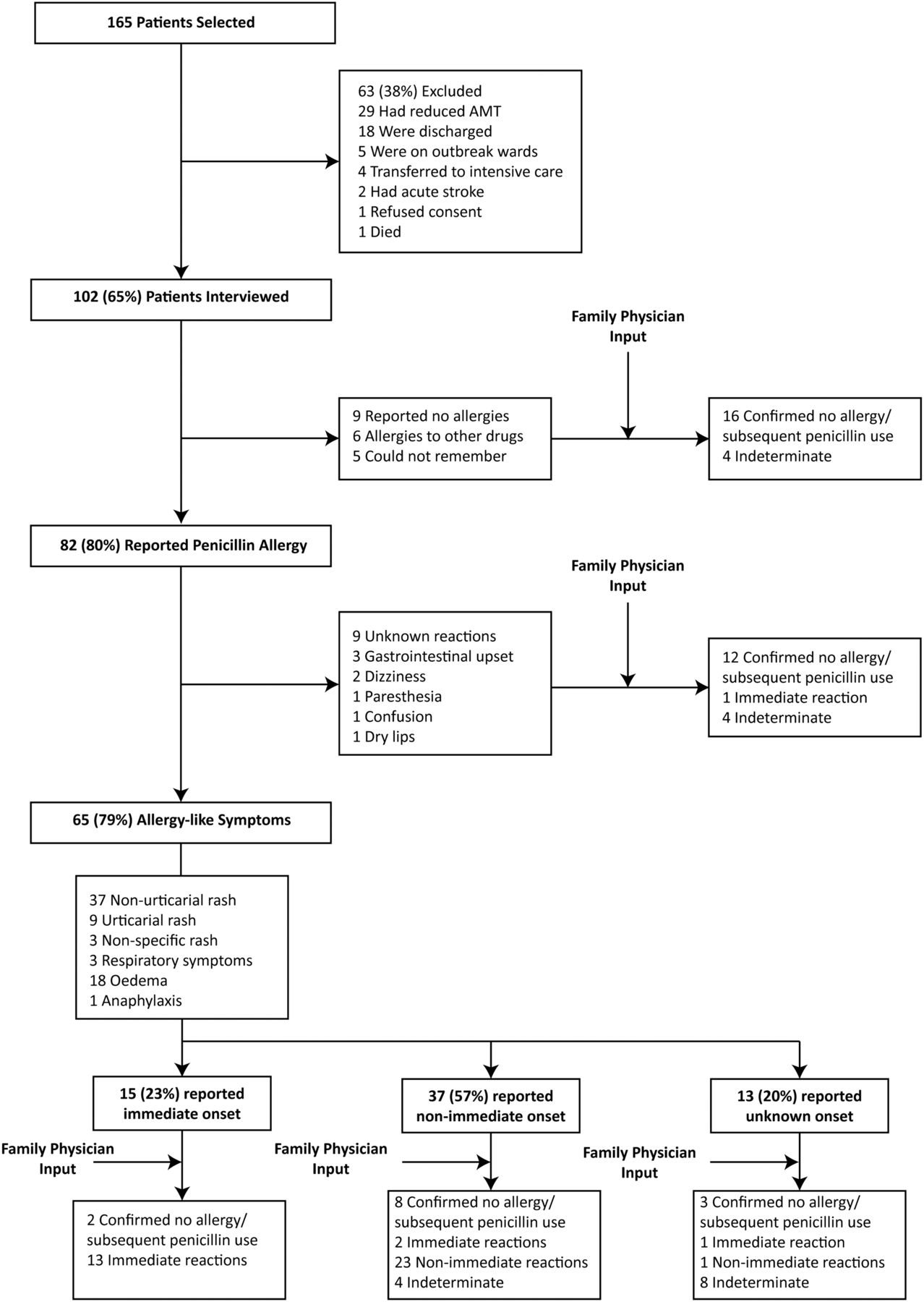
{kind=link}
Flow diagram of study patients and results of structured clinical history from patient and their family physician. AMT, Abbreviated Mental Test.
Clinical interpretation
A total of 102 patients (10%) from a total of 986 patients who were reported as penicillin allergic were assessed. Using a combination of information obtained from interviewing the patients and their family physicians, data suggested that 16 (16%) patients had a possible immediate (type 1) hypersensitivity to penicillin; 25 (24%) had possible non-immediate reactions; 41 (40%) patients were likely ‘non-allergic’ and in 20 (20%) patients the reaction to penicillin could not be clarified (‘indeterminate’).
Further details of the evaluation and categorisation of reactions are summarised in figure 1.
Cost analysis
Cost analysis is summarised in table 2.
Discussion
This is the first study from the UK investigating the pharmaco-economic implications of penicillin allergy. Our study has highlighted that the diagnosis of penicillin allergy is erroneous in a significant proportion of patients and that this could pose a major financial burden on the National Health Service. Previous studies from other countries, including a recent cohort study15 from North America, highlighted erroneous rates of penicillin allergy in hospitalised patients and a potential relationship between ‘penicillin allergy’ and higher rates of C difficile and longer hospital stays. Our study focuses on the financial implications of penicillin allergy and the potential for a more accurate diagnosis using structured clinical history alone per se.
In our study, 80% of patients with a diagnostic label of penicillin allergy claimed to be penicillin allergic when interviewed. Eleven per cent of these patients were not able to provide any details of the nature of the penicillin allergy. This is in contrast to other studies where 23.5%–66% of patients with an alleged allergy did not remember the nature of their reaction.16 ,17
We found that 31% of patients who had a label of penicillin allergy had been prescribed penicillin within the past year and 21% had penicillin after the date of their reaction. These figures are lower than the 34.3% and 48.5% penicillin re-prescribing rates found in previous studies.5 ,18
Combined analysis of data from interviews of patient and family physician suggested that the label of penicillin allergy was erroneous for at least 40% of the patients. This exceeds the 13% of patients who had their penicillin allergy excluded by thorough history alone in a previous study.19
Antibiotic costs were between 1.82-fold and 2.58-fold higher than if patients had used first-line antibiotics. This compares with the 2.3-fold higher cost and 1.5-fold to 1.7-fold higher costs found by Borch et al5 if only cases where antibiotics were indicated were included.
In the 40% of patients where the penicillin allergy label was considered erroneous, antibiotic costs were between 1.86-fold and 2.75-fold higher than if first-line antibiotics were used. This translated to a potential cost saving of between £5851.18 and £14 471.93 if these patients had their penicillin allergy label removed and had been prescribed first-line antibiotics.
Over the 3 months of the study, 8343 patients were prescribed antibiotics and 986 (12%) had a diagnostic label of penicillin allergy. Extrapolating these data would suggest that in HoEFT, 1577 patients over a year could have their diagnostic label of penicillin allergy excluded by structured history alone. This translates to a potential annual cost saving of between £225 056 and £556 640 for antibiotic acquisition alone. Cost analysis and overheads relating to additional days of hospital stay due to employment of second-line antibiotics, associated therapeutic monitoring and complications including C difficile infection and antibiotic resistance were not within the scope of this study and would potentially add to overall costs incurred due to false diagnostic label of penicillin allergy.
Six patients were tested positive for C difficile including three testing positive for C difficile toxin more than 48 h after admission. Three of these patients were found to be likely non-allergic to penicillin; one had non-immediate reaction to penicillin and two were indeterminate. Two had been prescribed fluoroquinolones but neither were classed as likely non-allergic after evaluation.
This is a pilot study and has some limitations. First, clinical history was not followed by allergy testing and drug provocation tests. However, in routine clinical practice, allergy can be excluded in patients based on clinical history and/or careful scrutiny of previous clinical records as well as liaison with the family physician. Also, immediate allergic reactions can be confirmed based on clinical history per se and allergy testing±provocative testing is not indicated. Allergy testing is usually considered in patients where there is paucity of information.
Second, patients were recruited prospectively but over a period of 3 months only and the study was restricted to working hours (9:00–17:00, Monday–Friday).
Third, 38% of the patients who were selected from the EP system had to be excluded from the study due to either reduced AMT scores or discharge from hospital before evaluation.
Fourth, due to time constraints and limitations within the EP system, this study could only give a cost range for the antibiotics used rather than the precise cost. This was because patients would be prescribed intravenous antibiotics and step down to oral formulations at varying times. Fifth, our study had a small sample size. Finally, in modern clinical practice, the time available to take a full medical history is limited. Hence, in patients who report penicillin allergy, a limited range of structured questions would help save medical staff time in categorising allergy status. This was not calculated in our study or the potential time needed to consult external teams such as microbiology/infectious diseases and allergy/immunology.
Allergy tests are not indicated in patients with a clear history of an immediate or non-immediate hypersensitivity reaction to penicillin. Investigations may be considered in patients where there is insufficient information relating to the ‘index reaction’. However, our data have highlighted a need for larger multicentre prospective randomised case–control studies to investigate the benefit and safety of formal allergy specialist evaluation (to exclude an allergy based on the structured approach employed in this study, and where needed supplemented with formal allergy testing) during the acute phase of hospital admission versus using alternative antibiotics and measuring endpoints such as rates of allergic reaction to administration of penicillin following exclusion of an allergy, 30-day mortality, antibiotic resistance and C difficile rates. This would allow for a more comprehensive health economic analysis to enable policymakers to make important decisions regarding management of infections in patients with a diagnostic label of penicillin allergy. Importantly there is an urgent need to improve documentation of adverse drug reactions by all physicians.
In conclusion, the diagnosis of penicillin allergy is erroneous in a significant proportion of patients and combination of a structured history from patient and their family physician is helpful in evaluation. Furthermore, costs of using second-line antibiotics are significantly higher.
Take home messages
-
There is growing evidence that penicillin-allergic patients treated with second-line antimicrobial agents have poorer outcomes including having higher rates of Clostridium difficile and longer hospital stays.
-
Many patients that report allergy to penicillin are proven to be non-allergic on formal immunological testing.
-
This prospective study showed 40% of penicillin allergy could be excluded using structured clinical history alone.
-
The cost of using second-line antibiotics in penicillin-allergic patients was calculated as 1.82-fold to 2.58-fold higher than first-line antibiotics. This shows the potential for substantial cost savings.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors ML has overall responsibility for content and contributed to the planning, conducting and reporting of the study. MTK and DP contributed to the planning and reporting of the study. SR contributed to the planning and conducting the study.
-
Competing interests MTK has received honorarium from Allergy Therapeutics. He is a member of National Clinical Reference Group for Specialised Clinical Allergy and Immunology Service.
-
Ethics approval This study was submitted to the clinical governance department of Heart of England NHS Foundation Trust. No patient identifiable information was included.
-
Provenance and peer review Not commissioned; externally peer reviewed.