Article Text

Abstract
As the population of older people is expanding and medication review is both time consuming and money consuming, a more sophisticated approach to improve patient medication use might be necessary. An integrated combination of several medication therapy management techniques might therefore more efficiently improve medication effectiveness, medication safety and also increase the efficiency Currently, pharmacists are involved in multiple, often seldom integrated, pharmaceutical care activities like (among others) medication formularies, medication guidelines, clinical rules and patient education and adherence counselling. A possible way to integrate these different activities is the medication therapy management pyramid proposed in this article. The base of the medication therapy management pyramid is population-based care, whereas the top of the pyramid is patient-centred care. When conducting possible interventions on population level and by the adequate use of medication surveillance systems and clinical rules during dispensing, a medication review will shift from a system repairing overdue maintenance to an individualised medication coaching consult.
- PHARMACOTHERAPY
Statistics from Altmetric.com
Medication safety has to be improved…
Medications are involved in 80% of all treatments and impact every aspect of a patient’s life.1 Although medications usually improve patients' quality and/or duration of life, they can also cause considerable harm. In US hospitals, for example, it is estimated that yearly 380 000–450 000 preventable adverse drug events occur (at a cost of $3.5 billion) and 7000 patients die due to medication errors.2 ,3 Also in Europe, the Dutch Hospital Admissions Related to Medication study revealed that 5.6% of all the acute hospital admissions were medication related. Almost half (46.5%) of these admissions were related to a medication error and therefore potentially preventable.4 These studies, and many others, confirm that medication safety has to be improved.5–7
…as well as medication adherence
Besides patient safety, medication use can also be improved by increasing patients' medication adherence. Reports of the WHO and the National Institute for Health and Care Excellence reveal that 30–50% of patients with chronic illnesses do not take their medication as prescribed.8 Consequences of non-adherence include worsening condition, increased comorbid diseases, increased healthcare costs and death.9 ,10
Medication review as possible instrument to reduce drug-related problems
Thus, interventions are warranted to improve the use of medication and better fulfil patients' drug-related needs, being (1) appropriate medication (right indication and matching patients' individual characteristics), (2) effective medication (most effective drug, right dose), (3) safe medication and (4) medication that the patient is willing to take.11
Medication reviews have been proposed, and introduced, as a method to improve patients' drug use and needs. It is defined as “a structured, critical examination of a patient's medicines with the objective of reaching an agreement with the patient about treatment, optimizing the impact of medicines, minimizing the number of drug-related problems (DRPs) and reducing waste”.12
Effectiveness of medication review is however not fully documented
Although there is a worldwide steady increase in performed medication reviews (partly due to the fact that in some countries guidelines recommend medication review in older patients), there is still debate on both the effectiveness and cost-effectiveness of medication review. Several meta-analyses and systematic reviews did not found an association between medication reviews and lower hospital admission rates, clinical outcomes or mortality in older patients.13 ,14 Medication review might possibly positively affect drug-related problems (DRPs), medication changes and drug load. However, insufficient data exist to know whether the latter increases patients’ quality of life. As the population of older people is expanding and medication review is both time consuming and money consuming, a more sophisticated approach to improve patients' medication use and medication safety is necessary.
Solving DRPs earlier during prescribing/dispensing, not during review
Furthermore, it is often recognised that DRPs detected in medication reviews (like adding gastroprotective agents to patients at risk using non-steroidal anti-inflammatory drugs (NSAIDs) and/or adding laxatives to opiate users) are in fact overdue maintenance. The omission of gastroprotectives or laxatives has to be discovered during prescribing and/or dispensing of NSAIDs and opiates, respectively. Intervening earlier, during the prescribing/dispensing phase, decreases the period that the patient is at risk for ulcers or constipation. In order to prevent overdue activities, proactive local guidelines to prevent DRPs should be defined for the whole target population and subsequently monitored by clinical rules. Thus, for example, by making local guidelines on NSAID gastroprotection and using clinical rules detecting abbreviations from these guidelines on a population basis, medication review will only rarely detect this DRP anymore.
The medication management pyramid: integrating different pharmaceutical care interventions
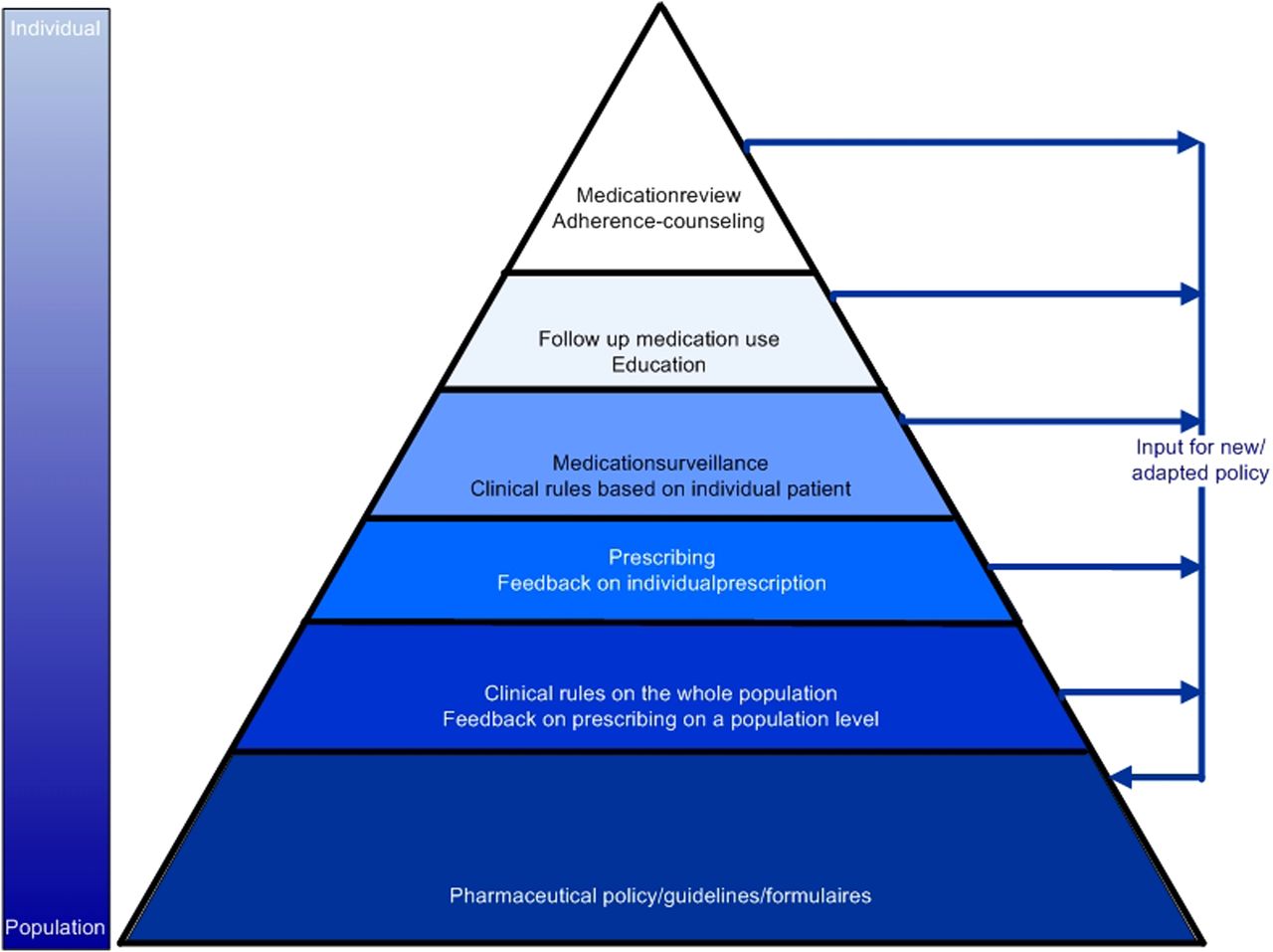
In fact, an integrated combination of several medication therapy management techniques might improve medication effectiveness, medication safety and also increase the efficiency (resulting in more pharmaceutical care). Currently, pharmacists are involved in multiple, often seldom integrated, pharmaceutical care activities like (among others) medication formularies, medication guidelines, clinical rules and patient education and adherence counselling. A possible way to integrate these different activities is the medication therapy management pyramid (figure 1).
{kind=link}
The medication therapy management pyramid: an integral approach of pharmaceutical care with population-based pharmaceutical care (pharmaceutical care guidelines/policy) as base of the pyramid. The more pharmaceutical care interventions are integrated in population-based pharmaceutical care (base of the pyramid), the more time will be available for more personalised pharmaceutical care (top of the pyramid).
Population pharmaceutical care
The base of the medication therapy management pyramid is population-based care, whereas the top of the pyramid is patient-centred care. Population care is often established in medication policy and medication guidelines. The extent of implementation can be monitored with population clinical rules followed by feedback to the prescribers. Population care is the most efficient care as one single guideline (monitored with a clinical rule) might manage the total population proactively. Executing population pharmaceutical care is neither time, patient nor prescription dependent. Drug formulary policies and prescribing preventive co-medication are suitable for population care.
Prescription and individual pharmaceutical care
In contrast to population care, medication surveillance during/after dispensing is done on an individual basis. However, clinical decision support systems (or clinical rules) might assist the pharmacy staff during dispensing. Besides detection of interactions and allergies, real-time clinical rules might monitor instantly whether the medication dosage is in accordance with patients' renal function. Or whether (in case the physician misses the population-based surveillance) the patient has the necessary medication to reduce side effects.
Population-based medication management saves time for individualised pharmaceutical care
When conducting possible interventions on population level and by the adequate use of medication surveillance systems and clinical rules during dispensing, a medication review will shift from a system repairing overdue maintenance to an individualised medication coaching consult. Based on patients' demographic (age, gender, race, weight), clinical (co-medication, comorbidity, experienced (side-) effects), psychological (beliefs about medication, acceptance of the disease) and social (spouse, children, work) characteristics, patients' medication use can be tailored to patients' individual situation, thereby increasing the effectiveness, safety and cost-effectiveness of patients' pharmacotherapy.
Pharmaceutical care will get in a continuous quality cycle
Finally, observation from the individualised care can be input for population care. Interventions to prevent frequently observed drug related in individual care can be implemented in population care. This creates a continuous quality cycle, encompassing plan (medication policy), do (prescriptions, clinical rules, medication reviews), check (prescription information, frequently observed DRPs during clinical rules and medication reviews) and act (incorporating new guidelines to prevent frequently occurring DRPs).
Key messages
What is already known
Medication review has been proposed, and introduced, as a method to improve patient’s drug use and needs.
However, sometimes some medication review activities are perceived as overdue maintenance.
As medication review is both time and money consuming, a more sophisticated approach to improve medication use might be necessary.
What this study adds
This article proposes an integrated combination of several medication therapy management techniques connected to each other in the medication management pyramid.
In the basis of the pyramid population based pharmaceutical care is grounded, whereas the top of the pyramid addresses patient-centred care.
Conducting interventions, when possible, on a population level, will shift medication review interventions from a system repairing overdue maintenance to an individualised medication coaching consult.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.