Article Text

Abstract
Objective Roux-en-Y gastric bypass (RYGB) surgery induces major changes in the gastrointestinal tract that may alter the pharmacokinetics of orally administered drugs. Results from pharmacokinetic studies are sparse. This study aimed to investigate the effect of RYGB on the bioavailability of metoprolol from immediate release (IR) and controlled release (CR) tablets in female patient volunteers before and after surgery.
Methods An explorative, two-phase, single oral dose pharmacokinetic study of metoprolol in female patients undergoing RYGB was carried out. The dose was administered twice in each patient, 1 month before and 6 months after surgery. After intake of either 100 mg of metoprolol IR or CR tablet serum concentration-time profiles of metoprolol were determined. The endpoint was the ratio of AUCafter/AUCbefore of metoprolol.
Results Twelve patients were included in the study (metoprolol IR: 7; metoprolol CR: 5). After intake of a metoprolol IR tablet major intraindividual and interindividual differences for area under the serum concentration versus time curve (AUC) of metoprolol before and after surgery were observed (range ratio AUC0–10 hours after/AUC0–10 hours before: 0.74–1.98). For metoprolol CR tablets a significant reduction in bioavailability of metoprolol was observed after surgery (range ratio AUC0–24 hours after/AUC0–24 hours before: 0.43–0.77).
Conclusion RYGB may influence the bioavailability of metoprolol from an IR tablet. The magnitude of changes in bioavailability after RYGB requires close monitoring of patients using metoprolol IR tablets and dose adjustment if deemed necessary. RYGB clearly reduces the bioavailability of metoprolol from a CR tablet. After RYGB clinicians may consider to increase the dose according to clinical response.
- gastric bypass surgery
- bioavailability
- metoprolol
- pharmacokinetics
- immediate release
- controlled release
Statistics from Altmetric.com
Introduction
In 2014 Roux-en-Y gastric bypass (RYGB) was the second most commonly performed bariatric procedure in the world.1 RYGB achieves weight loss through restriction of food intake, altered neurohormonal signalling in body weight regulation, increased energy expenditure and altered bile salt metabolism due to changes in the gut microbiome. True malabsorption is rare after RYGB, but changes in anatomy and function such as a reduced gastric volume, increased gastric pH, altered gastric emptying, reduced intestinal surface area for absorption, changed intestinal and hepatic first-pass metabolism, shorter intestinal transit time and more distal delivery of bile and pancreatic secretions may all affect the absorption and thus the bioavailability of orally administered drugs.2–4 After RYGB the performance of oral formulation types such as slow release or delayed release may suffer from critical changes affecting adequate drug absorption and thereby their efficacy.5
Generally after restrictive-malabsorptive procedures, such as RYGB, it is recommended to substitute controlled release (CR) drug formulations into immediate release (IR) dosage forms.6 This is reflected in the European guidelines on metabolic and bariatric surgery, stating that in the follow-up after bariatric surgery, patients should be advised to preferably use crushed and/or rapid release medication.7 However, these recommendations are not evidence based. So far, only a few studies have been published on the influence of RYGB on the pharmacokinetics of drugs, showing large variations. Moreover, changes are characterised by high unpredictability.8 Therefore, more studies are needed on the influence of RYGB on the pharmacokinetic behaviour.9
Bariatric surgery reduces the risk factors for cardiovascular disease. This influences the use of medication. After restrictive-malabsorptive weight loss procedures, such as RYGB, a significant reduction in use of beta-blockers has been reported, nonetheless a considerable number of patients still use a beta-blocker.10 11 Metoprolol, a lipophilic cardioselective β1-adrenoreceptor antagonist, has a long history of use in the treatment of hypertension, angina pectoris and other cardiovascular diseases, as well as for the prophylactic treatment of migraine. It is available as IR and CR tablet. After oral administration, absorption of metoprolol from the gastrointestinal tract is almost complete. Due to first-pass hepatic metabolism, about 50% of the dose reaches the systemic circulation. In the liver metoprolol is metabolised for 70%–80% by cytochrome P450 2D6 (CYP2D6) into several metabolites. Alpha-hydroxymetoprolol is an active metabolite, possessing only around one-tenth of the β1-blocking activity of metoprolol. It is formed by CYP2D6, making it a suitable marker for CYP2D6 activity.12 13 In urine approximately 7% of the administered dose of metoprolol is recovered as α-hydroxymetoprolol. Serum concentrations of α-hydroxymetoprolol vary depending on age and on the oxidation phenotype.13 14
The aim of the present study was to investigate the effect of RYGB on the bioavailability of metoprolol and formation of its metabolite α-hydroxymetoprolol, after a single oral dose of metoprolol IR and CR tablet in female bariatric surgery patient volunteers before and after surgery.
Methods
Participants
The study was conducted in female patients undergoing RYGB. Only female patients were enrolled in this study, since for metoprolol gender-related differences exist in the pharmacokinetics leading to greater drug exposure (higher Cmax and area under the serum concentration versus time curve (AUC)) for women than men.15 Moreover, almost 80% of the patients undergoing bariatric surgery is female.16 The criteria for enrolment in this study were: female, age between 18 and 50 years, non-smokers, physiologically normal liver and kidney function, a normal ECG and extensive or intermediate CYP2D6 metaboliser status, as evidenced by genotyping. Pregnant patients, patients who had previously undergone gastrointestinal surgery and patients currently receiving metoprolol or with contraindications to treatment with metoprolol were excluded. Patients suffering from dumping syndrome after surgery were also excluded. After having given written informed consent the subjects underwent a medical examination by an internal medicine specialist. Genotyping was performed using TaqMan real-time PCR (LightCycler 480, Roche, Basel, Switzerland) and translated to a CYP2D6 predicted phenotype.17 Only patients meeting all criteria participated in the study, seven in the metoprolol IR and five in the metoprolol CR part. All subjects underwent RYGB surgery resulting in the creation of a gastric pouch with a volume of 20–70 mL, a biliopancreatic limb of 80–150 cm and an alimentary limb of 150 cm. In this study, subjects were their own control, taking the same tablet formulation of metoprolol before and after RYGB. Patients were allowed to participate in the IR and CR part of the study with an interval of at least 7 days between administrations of the two formulations of metoprolol.
Metoprolol
In the present study the bioavailability of metoprolol from two different oral tablet formulations before and after RYGB was investigated. Metoprolol tartrate 100 mg IR tablet (Pharmachemie, Haarlem, The Netherlands (metoprolol IR)), and metoprolol succinate 95 mg CR tablet, equivalent to 100 mg of metoprolol tartrate (Pharmachemie (metoprolol CR)) were used.
Study design
An explorative, two-phase single oral dose pharmacokinetic study of metoprolol was performed. A metoprolol IR or CR tablet was administered twice to each patient, 1 month before and 6 months after surgery. After an overnight fast of at least 10 hours subjects came to the clinical research unit of the hospital. Usual medication of the patients was adjusted in a way that interference with the study was prevented and that the patient’s treatment was guaranteed. After insertion of a peripheral intravenous cannula participants ingested a metoprolol IR or CR tablet with 150 mL water (presurgery), or with as little water as possible (postsurgery). Blood samples were collected at 0, 0.5, 1, 1.5 (only IR), 2, 3, 4, 5, 6, 8, 10 and 24 (only CR) hours after intake. After the 10 hours blood sample was taken, subjects were allowed to go home. For subjects taking metoprolol CR a 24-hour blood sample was taken at the patient’s home. Within 2 hours after collection blood samples were centrifuged for 10 min at 2000 g at 4°C and serum samples were stored at –24°C until analysis. A standardised snack and standardised meals were served 2, 4 and 10 hours after administration of the tablet, respectively. During the first 6 hours after intake of the medication the patients were not allowed to lie down. For safety reasons blood pressure and heart rate were regularly monitored. Concentrations of metoprolol and its metabolite α-hydroxymetoprolol were determined by means of a validated LC-Orbitrap MS method.18 The lower limit of quantitation of the assay was 2.0 ng/mL for metoprolol and 1.0 ng/mL for α-hydroxymetoprolol, respectively. Four months after surgery, before the start of the second phase of the study, the patients were asked about dumping syndrome symptoms by means of a questionnaire.19 Complications of the surgery which might interfere with the study were also assessed. The subject was withdrawn from the study if she was suffering from the dumping syndrome or from interfering complications.
Pharmacokinetic parameters
The following pharmacokinetic parameters of metoprolol and α-hydroxymetoprolol were determined: maximum concentration (Cmax), time to maximum concentration (Tmax) (metoprolol IR only) and AUC for 10 (metoprolol IR) or 24 hours (metoprolol CR). The areas under the serum concentration versus time curves (AUC0–10 hours or AUC0–24 hours) were determined using the linear trapezoidal rule in Microsoft Excel (2013). The endpoint was the ratio AUCafter/AUCbefore of metoprolol and α-hydroxymetoprolol for each participant. A paired t-test was performed on the obtained data before and after surgery. A p value <0.05 was considered significant.
Results
Seven patients were included in the metoprolol IR part of the study, five patients in the metoprolol CR part. Two patients participated in both studies.
In table 1 the characteristics of the participants of the pharmacokinetic study are shown. After intake of the single dose of metoprolol no side effects were reported. After surgery no complications from the gastric bypass surgery which might interfere with the study occurred and the participants did not suffer from symptoms of the dumping syndrome. No subjects were withdrawn from the study.
Characteristics of study participants
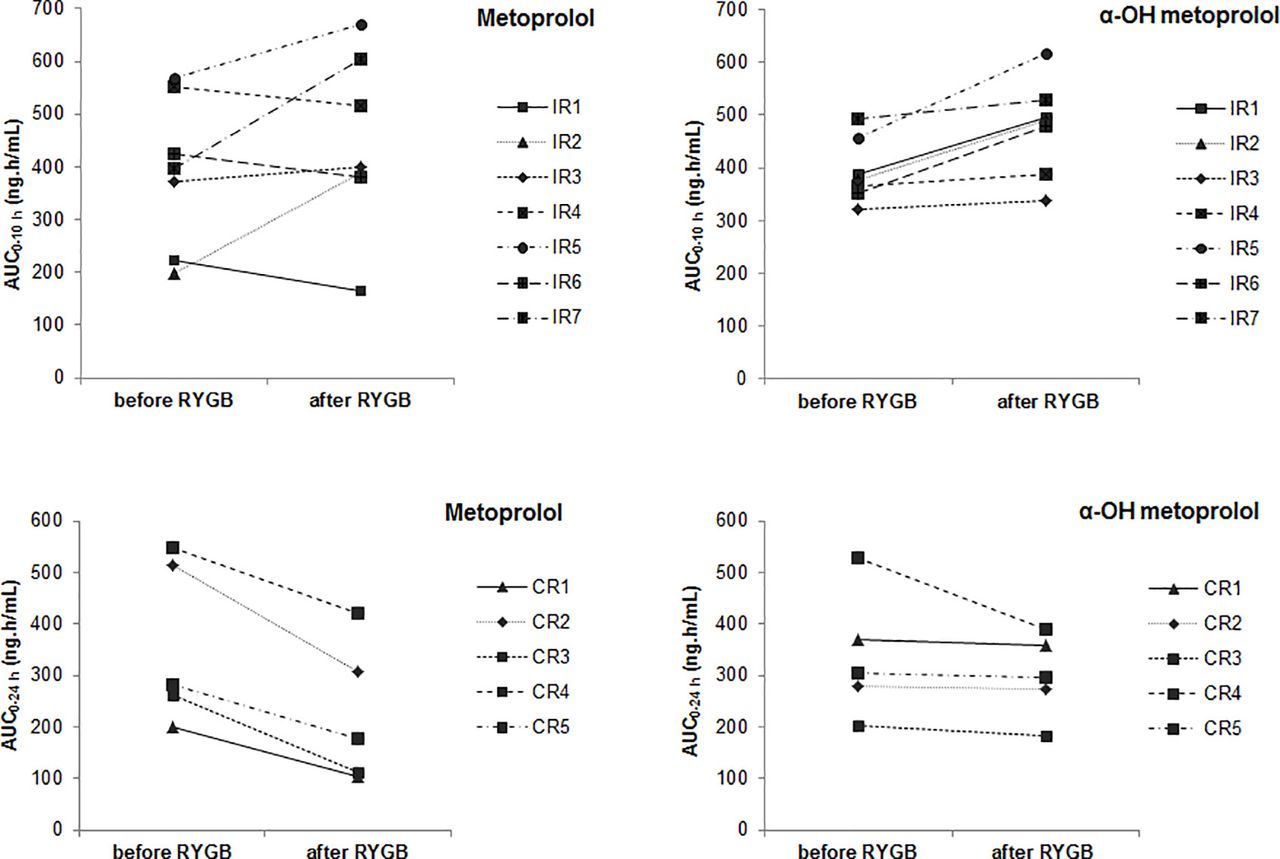
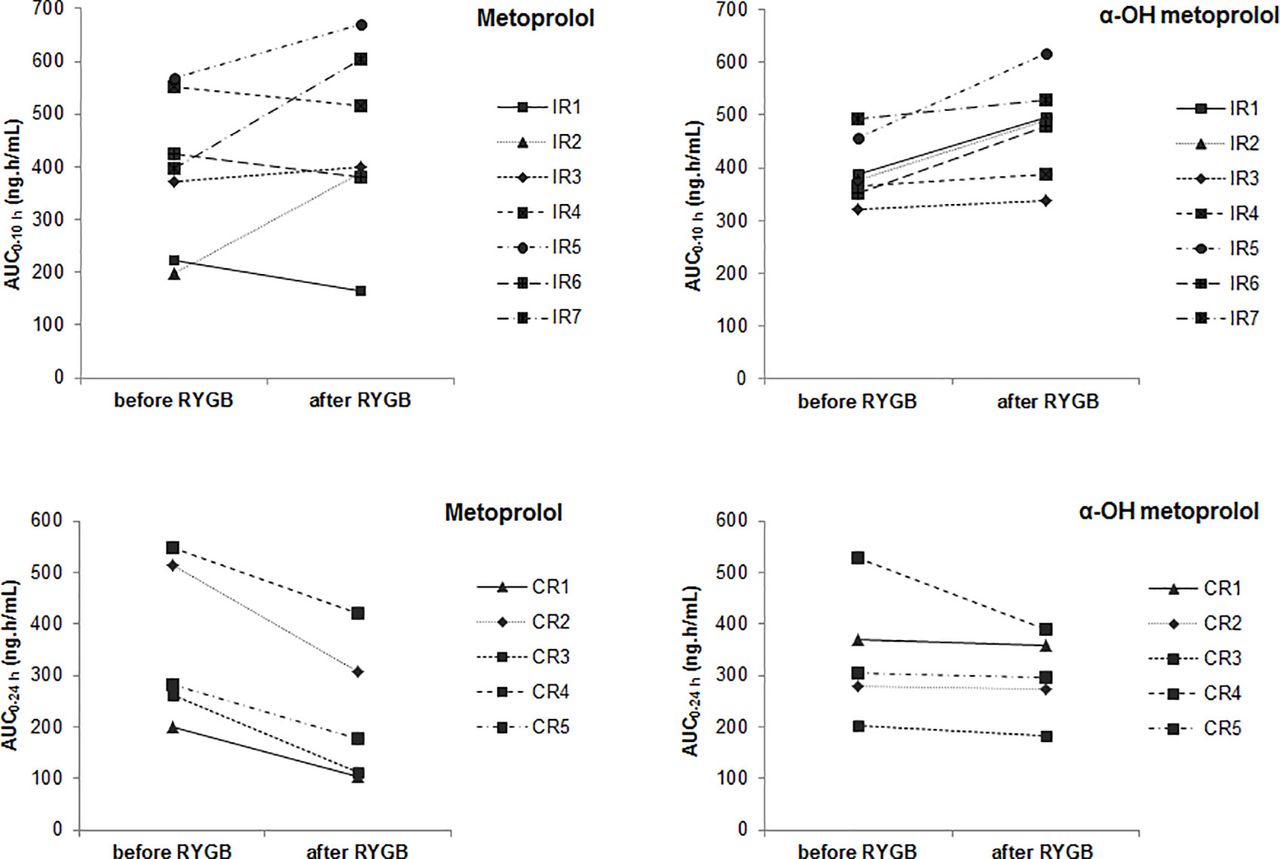
In table 2 pharmacokinetic parameters after intake of metoprolol IR and CR, respectively, before and after RYGB are presented. Online supplementary appendix figures A1 and A2 display the individual serum concentration-time profiles of metoprolol and α-hydroxymetoprolol after administration of either a single dose of metoprolol IR or CR, respectively, before and after RYGB. Figure 1 shows the change in AUC of metoprolol and α-hydroxymetoprolol for individual participants, after administration of metoprolol IR and CR, respectively, before and after RYGB.
Pharmacokinetic parameters after administration of a single oral dose of metoprolol tartrate 100 immediate release (IR) tablet (seven participants) and metoprolol succinate 95 mg controlled release (CR) tablet (five participants)
{kind=link}
AUC0–10 hours after administration of a single oral dose of metoprolol tartrate 100 mg immediate release (IR) tablet (upper windows) and AUC0–24 hours after administration of a single oral dose of metoprolol succinate 95 mg controlled release (CR) tablet (lower windows) before and after Roux-en-Y gastric bypass (RYGB). AUC, area under the serum concentration versus time curve.
After intake of metoprolol IR tablet metoprolol exposure, Cmax and Tmax were not significantly altered by RYGB. However, large intraindividual and interindividual differences for AUC of metoprolol (range ratio AUCafter/AUCbefore: 0.74–1.98), as well as for Cmax and Tmax were observed before and after surgery. The metabolite α-hydroxymetoprolol had a greater, significant exposure after RYGB (p=0.01). In Cmax a significant increase was also seen (p=0.01).
After intake of metoprolol CR tablet a significant reduction in bioavailability of metoprolol was observed (p<0.01; range ratio AUCafter/AUCbefore: 0.43–0.77). For α-hydroxymetoprolol the difference in exposure was not significant, with ratios of AUCafter/AUCbefore ranging from 0.74 to 0.98.
For both metoprolol IR and CR extensive metabolisers for CYP2D6 had an AUC for metoprolol in the lower range, before as well as after surgery.
Discussion
This study found that RYGB may influence the bioavailability of metoprolol from IR tablets. Large interindividual differences in the ratios of AUCafter/AUCbefore of metoprolol were observed. After intake of an IR tablet exposure of metoprolol after RYGB may be reduced or increased. For the individual patient the consequences of RYGB for dosing metoprolol IR tablets cannot be predicted. The magnitude of changes in bioavailability after RYGB requires close monitoring of patients using metoprolol IR tablets and dose adjustment if deemed necessary.
The bioavailability of metoprolol from CR tablets is reduced after RYGB. Therefore, after RYGB clinicians may consider to increase the dose according to clinical response.
Several factors that might affect bioavailability of metoprolol after RYGB should be considered. Metoprolol has been classified as a Biopharmaceutics Classification Scheme class I substance, having a high solubility and a high intestinal permeability, meaning that metoprolol will be easily dissolved and absorbed.20 Metoprolol is not absorbed from the stomach, but may be well and similarly absorbed throughout the small intestine and colon. Thus, metoprolol administered as an oral formulation is expected to be absorbed from any region of the intestine in which it is released.21–23 After RYGB the duodenum and proximal jejunum are no longer available for absorption, so reduced absorption may occur. In obese patients metoprolol, being a liposoluble compound, was found to have a higher volume of distribution with a lower Cmax compared with non-obese patients.24 With a decreased body mass index and body fat percentage after RYGB, one might expect a higher bioavailability.
Before enrolment in the study, participants were genotyped for CYP2D6 and poor metabolisers were excluded from participation. More intermediate than extensive metabolisers were included. This may be coincidence and due to the small numbers of inclusion. Although after RYGB after intake of a metoprolol IR tablet exposure of metoprolol was either reduced or increased for α-hydroxymetoprolol a significant increase in AUC was observed. (Patho)physiological alterations associated with obesity may have a specific impact on drug metabolism and elimination. Brill et al 25 found that in literature few studies indicate trends towards increased CYP2D6-mediated metabolites in obese versus non-obese patients. However, Abdussalam et al 26 showed that in rats given a high-fat diet CYP2D1 (the equivalent in rat to human CYP2D6) is downregulated. Higher levels of α-hydroxymetoprolol after RYGB might be caused by increased CYP2D6 metabolism due to weight loss. After intake of a metoprolol CR tablet bioavailability of metoprolol was reduced, but, except for one patient, no reduction in AUC was observed for α-hydroxymetoprolol after RYGB. Lower exposure of metoprolol after RYGB did not lead to lower levels of α-hydroxymetoprolol. This might be caused by increased CYP2D6 metabolism due to weight loss after RYGB.
As might be expected, extensive CYP2D6 metabolisers participating in this study showed a bioavailability of metoprolol in the lower range before as well as after RYGB. However, after intake of a metoprolol IR tablet, a decrease as well as an increase in bioavailability after RYGB was observed, depending on the subject.
In the present study after RYGB decreased bioavailability of metoprolol from CR tablet is observed. In normal patients systemic availability of CR metoprolol formulations is 20%–30% lower than that after administration of an IR tablet.14 According to Plosker and Clissold,14 the reduction in bioavailability is likely related to the relatively slow rate of drug delivery which enhances presystemic clearance of metoprolol because hepatic extraction is a saturable process. Moreover, since transit time through the gastrointestinal tract can vary, some active drug may remain in the CR preparations at the time they are eliminated from the body. This might also contribute to reduced systemic availability in some patients. After RYGB, intestinal transit time might be a limiting factor for absorption from a CR formulation. However, data on intestinal transit time after RYGB are sparse and conflicting. Using a sulfasalazine tablet as a marker, Carswell et al 27 found no influence of RYGB on orocaecal transit time. Dirksen et al 28 showed that 1.5 years after RYGB pouch emptying time was shorter after a meal, but small intestinal transit was slower in patients than in control subjects. Colonic transit time did not differ. In patients 5.7 years after RYGB Nguyen et al 29 found that pouch emptying and caecal arrival time were more rapid compared with control subjects. Pouch emptying tended to be faster after 150 mL than after 50 mL drinks. In bioavailability studies oral tablet formulations are usually ingested with 150 mL of water. Because we did not want pouch emptying be influenced by the ingested volume of water, we decided to administer the metoprolol IR and CR tablets with 150 mL of water before surgery and with as little water as possible after surgery.
Possible variations in absorption of metoprolol after RYGB might be caused by changes in release from the oral tablet formulations. In vitro dissolution experiments showed that release patterns of metoprolol from IR and CR tablets in simulated RYGB conditions did not differ from those found in conditions before RYGB. Under all conditions applied, metoprolol IR and CR tablets showed adequate dissolution, fully complying with pharmacopoeial requirements.30 From this, we conclude that the observed changes in bioavailability of metoprolol after RYGB are not caused by changes in release rate of metoprolol from the studied IR and CR tablet formulations as a result of environmental conditions.
As yet, for some drugs the influence of RYGB on pharmacokinetic properties has been evaluated in controlled clinical studies. However, well-designed clinical studies with repeated measures before and after surgery are scarce and not all effects of RYGB on drug exposure reported so far are of clinical importance.8 9 31 An example of a well-designed study is the repeated measure study by Mitrov-Winkelmolen et al.32 They found a faster absorption of both acetylsalicylic acid and omeprazole after RYGB with a higher exposure of acetylsalicylic acid and an average decrease in bioavailability of omeprazole. Their findings have consequences for the dosing of omeprazole after RYGB (increase the dose in patients with inadequate response), but not for acetylsalicylic acid.
Gesquiere et al 33 performed a single-dose pharmacokinetic study of metoprolol tartrate 200 mg IR and CR formulations in 14 healthy volunteers before and 6–8 months after RYGB. They concluded that the oral exposure of metoprolol from immediate and controlled-release formulations was not significantly different after RYGB compared with before, although there was a tendency towards higher exposure after surgery. This different outcome compared with the results from our study may be explained in terms of different design in the Gesquiere et al’s study. Women (10) as well as men (4) were included. Before inclusion the CYP2D6 genotype of the patients was not determined. In addition, no individual data were presented, only mean AUC0–24 hours with 95% CI. Serum concentrations of metabolites of metoprolol were not measured. After RYGB participants ingested the tablets with 150 mL of water. By drinking this volume, pouch emptying might be accelerated.29 Moreover, in daily practice patients may not swallow a tablet with such a volume of water.
This study has several limitations. The sample sizes of the metoprolol IR and CR part of the study were small. The findings of this study may have implications for dosing metoprolol after RYGB, despite the fact that this was an explorative pharmacokinetic study. Only women were included in this study. Although pharmacokinetics of metoprolol is different in women compared with men, the effects of RYGB on bioavailability of metoprolol after oral administration in men might be comparable. After surgery this study was performed 6 months after RYGB. Relatively soon after surgery or in the long term results might have been different. After RYGB intestinal adaptation may occur, where mucosal hypertrophy within the remaining intestine gives an increase in absorptive capacity over time. It is unknown, however, whether intestinal adaptation affects absorption.4 Pharmacodynamics and pharmacokinetics of metoprolol are stereospecific. Metoprolol is used as a racemate. However, the assay used in this study was not enantioselective for metoprolol. Generally, beta-blockers are absorbed from the gastrointestinal tract via passive diffusion. Therefore, their absorption is not considered stereoselective.34
Conclusions
RYGB may influence the bioavailability of metoprolol from an IR tablet. After RYGB clinicians may consider to adjust the dose according to clinical response. RYGB reduces the bioavailability of metoprolol from a CR tablet. After RYGB clinicians may consider to increase the dose according to clinical response.
What this paper adds
What is already known on this subject
Roux-en-Y gastric bypass (RYGB) induces major changes in the gastrointestinal tract that may alter the pharmacokinetics of orally administered drugs.
Results from pharmacokinetic studies are sparse.
What this study adds
After RYGB possible changes in bioavailability of metoprolol from immediate release tablets require close monitoring of patients, with dose adjustment if necessary.
Because of reduced bioavailability of metoprolol from controlled release tablets after RYGB, the dose may be increased, according to clinical response.
Supplemental material
Supplemental material
Acknowledgments
We thank Berend Oosterhuis, PharmD, PhD†, for his fruitful discussions and ideas for setting up the study, and Daan J Touw, PharmD, PhD (Department of Clinical Pharmacy and Pharmacology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands) for his review of the results of the study. († deceased)
References
Footnotes
EAHP Statement 4: Clinical Pharmacy Services.
Contributors Study concept and design: JPY, ENvR, JTMW, BW, HWF, HJW. Acquisition of data: JPY, BO, JAA, ME, ERET, ECB, FLU. Analysis and interpretation of data: JPY, ENvR, BW, HWF, HJW. Drafting of the manuscript: JPY. Critical revision of the manuscript for important intellectual content: all authors. Study supervision: JPY, ENvR.
Funding This study was funded by a grant from the Science Fund (Wetenschapsfonds) Medical Centre Leeuwarden.
Competing interests None declared.
Ethics approval The regional research ethics committee reviewed and approved this study with EudraCT numbers 2013-002260-10 and 2013-002274-41.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.